Introduction
The pterygoid plexus is a complex of veins located in the infratemporal fossa of the skull with comprehensive connections to surrounding veins and anatomical structures. Bordering the pterygoid plexus are the medial and lateral pterygoid muscles along with the temporalis muscle, while the maxillary artery is surrounded by the plexus. As a result, the tributaries of the venous plexus parallel the branches of the maxillary artery. A clinically significant attribute of the pterygoid plexus is its communication with the cavernous sinus, the inferior ophthalmic vein, and the facial vein. Due to these communications, one must be aware of the potential to spread infection through the venous system into the cranial cavity. In addition, one must understand the anatomy of the infratemporal fossa and the pterygoid plexus when administering a block injection of the posterior superior alveolar nerve due to the risk of penetration and potential hematoma formation.[1][2]
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The boundaries of the infratemporal fossa with the pterygoid plexus sitting within divide into six landmarks. The posterior surface of the maxilla marks the boundary anteriorly, the tympanic plate and styloid process posteriorly, the ramus of the mandible laterally, the lateral pterygoid plate medially, medial pterygoid muscle attached to the medial surface of the ramus inferiorly. Finally, superior boundaries include the infratemporal surface of the greater wing of the sphenoid as well as the temporal fossa. The pterygoid plexus drains the nasal cavity, paranasal sinuses, and nasopharynx, to name a few, and contains tributaries correlating with the branches of the maxillary artery including the superior and inferior alveolar vein, sphenopalatine, deep temporal, and buccal veins to name a few. Posteriorly, the pterygoid plexus drains via the maxillary vein. The maxillary vein joins the superficial temporal vein to become the retromandibular vein and eventually drain into the external jugular vein upon combining with the posterior auricular vein. Similarly, the pterygoid plexus communicates with the facial vein through the deep facial vein as well as communication with the inferior ophthalmic vein through the inferior orbital fissure. The pterygoid plexus also communicates with the cavernous sinus in the cranial cavity by an emissary vein through foramen ovale.[1][3][4][5]
The pterygoid plexus functions to return the blood to the heart; this occurs during the movement of the lateral pterygoid, generating a pumping action of the blood back to the heart.
Embryology
The first vein of the face and neck that arises during embryological development is the ventral pharyngeal vein. This vein drains into the common cardinal vein. The primitive maxillary vein is located superolateral to the ventral pharyngeal vein and forms an anastomosis with the linguofacial vein. The resulting vein formed is the anterior facial vein. Upon further development of the embryo, the external jugular vein manifests from neck tissue and creates an anastomosis with the anterior facial vein. As development progresses, the external jugular vein will connect anteriorly with the facial vein and posteriorly with the retromandibular vein.[6]
Blood Supply and Lymphatics
Even though there are no lymphatics directly associated with the pterygoid plexus, the superficial cervical lymph nodes follow the external jugular vein, which is the vein into which the pterygoid plexus eventually drains. The superficial cervical lymph nodes divide to the superficial anterior and posterior-lateral superficial cervical lymph nodes. The posterior lateral lymph nodes are near the external jugular vein. Finally, the parotid group of lymph nodes is in close relation to the infratemporal fossa and the pterygoid plexus.[3]
Nerves
A 1984 study illustrates how some tributary veins of the pterygoid venous plexus can follow the lingual nerve.
Muscles
There is a close relationship of the venous plexus with the lateral pterygoid muscle and, to a lesser extent, with the medial pterygoid muscle.
Surgical Considerations
Procedures of the head and face must be done carefully due to complex anatomy and critical structures that lie in close proximity to one another. Understanding the anatomy and surrounding structures is imperative to prevent surgical complications of the region of the pterygoid plexus. A common nerve block given when working on posterior maxillary teeth is the posterior superior alveolar nerve block. Due to the location of the posterior superior alveolar foramen, which is the target of the nerve block, if one is not careful, the pterygoid plexus can be punctured, along with the maxillary artery and posterior superior alveolar nerve. The result of this is the formation of a hematoma.[7]
A crucial surgical consideration of the pterygoid plexus and the region surrounding it is the proximity and connection to the cavernous sinus. Upon performing a procedure, usually due to a dental infection, it is critical to ensure the infection's proper removal with no perforations leading to the infratemporal fossa and pterygoid plexus are present. Lastly, it is essential to use sterile equipment when performing surgery to prevent any infection of the tissue and area and potential complications.[3]
Clinical Significance
The pterygoid plexus has great clinical significance when dealing with infections. Due to its relation with the cavernous sinus, disseminated infection can drain into the cavernous sinus in the cranial cavity and cause a multitude of problems. Cavernous sinus thrombosis is a major complication that can be fatal if left untreated. This process occurs by embolization of bacteria, enabling the formation of thrombosis. The resulting thrombosis can potentially trap the bacteria in the sinus, creating further complications. Also, thrombosis blocks the normal drainage of the veins of the face causing periorbital edema, among other clinical signs. Compression of contents of the cavernous sinus can lead to neuropathy of cranial nerves III, IV, V1, V2, and VI. Major symptoms include cranial nerve VI palsy, diplopia, ophthalmoplegia, and paresthesias of the upper face covered by the ophthalmic and maxillary branches of the trigeminal nerve. Furthermore, cavernous venous thrombosis can potentially spread to the central nervous system. Since there are no valves in the cavernous system, the venous blood can spread to dural sinus and cerebral vein, potentially causing meningitis, brain abscess, or a stroke.[8][1][3][9]
Lastly, if damage occurs to the pterygoid plexus, the maxillary artery, or any vessels nearby, a hematoma can present. This damage is usually self-limiting and best treated with ice, compression, and rest. All in all, the complex anatomy and relations of the pterygoid plexus requires thorough knowledge and understanding of the region as well as caution and careful maneuvering when operating within this region.[10][11]
Other Issues
Congestion of the venous plexus and with an increase in volume could induce patulous eustachian tube symptoms.[12]
Media
(Click Image to Enlarge)
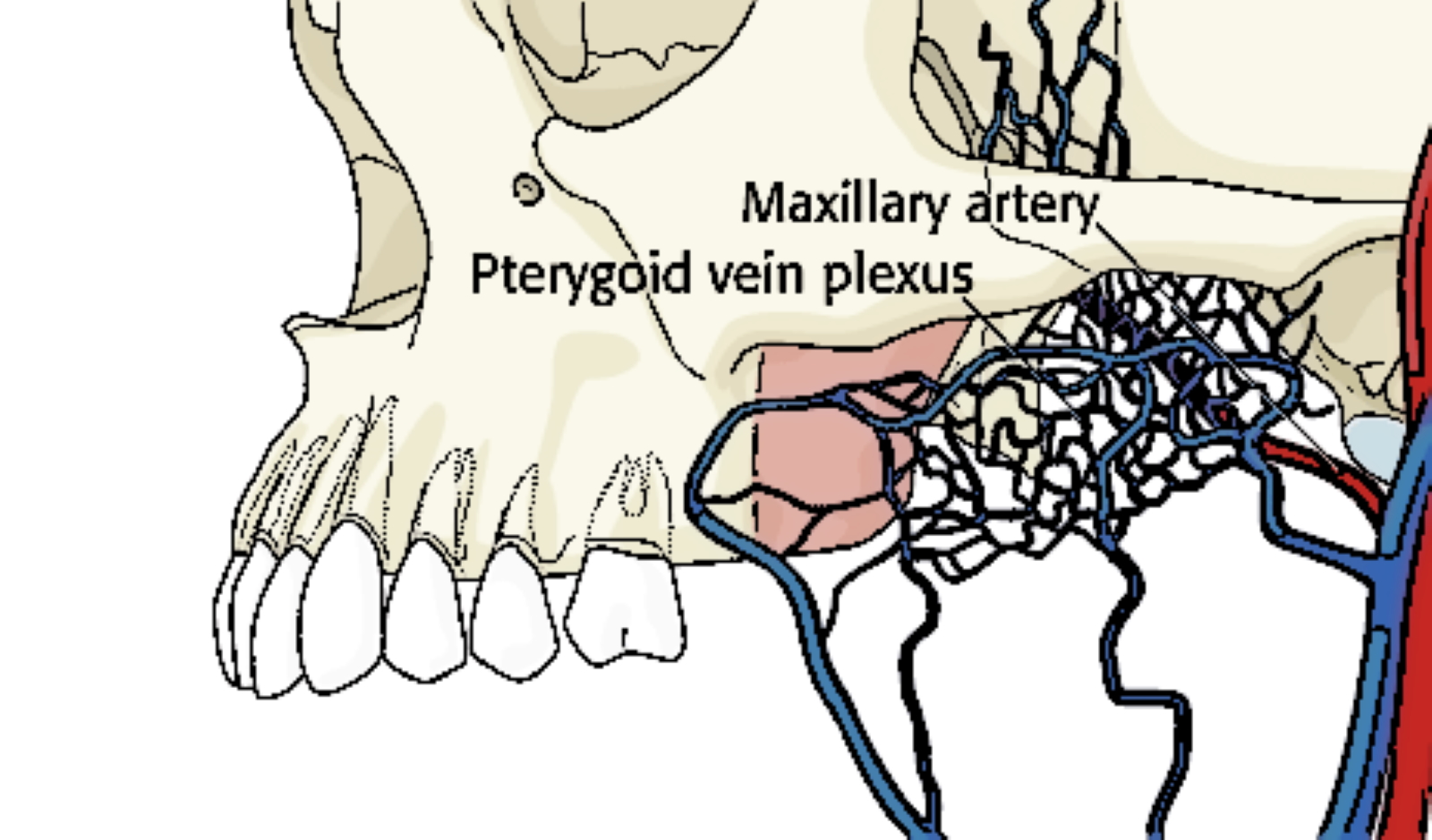
The figure shows the pterygoid venous plexus. Contributed by Bruno Bordoni, PhD.
References
Gofur EM, Al Khalili Y. Anatomy, Head and Neck: Internal Maxillary Arteries. StatPearls. 2023 Jan:(): [PubMed PMID: 31194441]
Jain V, Ellingson AN, Smoker WR. Lateral pterygoid muscle rhabdomyolysis. AJNR. American journal of neuroradiology. 2007 Nov-Dec:28(10):1876-7 [PubMed PMID: 17898189]
Level 3 (low-level) evidenceGermann AM, Jamal Z, Al Khalili Y. Anatomy, Head and Neck, Scalp Veins. StatPearls. 2023 Jan:(): [PubMed PMID: 31082005]
Casale J, Bordoni B. Anatomy, Head and Neck: Infratemporal Fossa. StatPearls. 2023 Jan:(): [PubMed PMID: 30725719]
Natsis K, Piagkou M, Repousi E, Tegos T, Gkioka A, Loukas M. The size of the foramen ovale regarding to the presence and absence of the emissary sphenoidal foramen: is there any relationship between them? Folia morphologica. 2018:77(1):90-98. doi: 10.5603/FM.a2017.0068. Epub 2017 Jul 13 [PubMed PMID: 28703850]
Mitsuhashi Y, Hayasaki K, Kawakami T, Nagata T, Kaneshiro Y, Umaba R, Ohata K. Dural Venous System in the Cavernous Sinus: A Literature Review and Embryological, Functional, and Endovascular Clinical Considerations. Neurologia medico-chirurgica. 2016 Jun 15:56(6):326-39. doi: 10.2176/nmc.ra.2015-0346. Epub 2016 Apr 11 [PubMed PMID: 27063146]
Thangavelu K, Kumar NS, Kannan R, Kumar JA. Simple and safe posterior superior alveolar nerve block. Anesthesia, essays and researches. 2012 Jan-Jun:6(1):74-7. doi: 10.4103/0259-1162.103379. Epub [PubMed PMID: 25885507]
Plewa MC, Tadi P, Gupta M. Cavernous Sinus Thrombosis. StatPearls. 2023 Jan:(): [PubMed PMID: 28846357]
Fabre C, Atallah I, Wroblewski I, Righini CA. Maxillary sinusitis complicated by stroke. European annals of otorhinolaryngology, head and neck diseases. 2018 Dec:135(6):449-451. doi: 10.1016/j.anorl.2018.07.004. Epub 2018 Jul 30 [PubMed PMID: 30072286]
Biočić J, Brajdić D, Perić B, Đanić P, Salarić I, Macan D. A Large Cheek Hematoma as a Complication of Local Anesthesia: Case Report. Acta stomatologica Croatica. 2018 Jun:52(2):156-159. doi: 10.15644/asc52/2/9. Epub [PubMed PMID: 30587858]
Level 3 (low-level) evidenceYue BYT, Zinn R, Roberts R, Wilson J. Use of thrombin-based haemostatic matrix in head and neck reconstructions: a potential risk factor for pulmonary embolism. ANZ journal of surgery. 2017 Dec:87(12):E276-E280. doi: 10.1111/ans.13618. Epub 2016 Aug 3 [PubMed PMID: 27490907]
Oshima T, Ogura M, Kikuchi T, Hori Y, Mugikura S, Higano S, Takahashi S, Kawase T, Kobayashi T. Involvement of pterygoid venous plexus in patulous eustachian tube symptoms. Acta oto-laryngologica. 2007 Jul:127(7):693-9 [PubMed PMID: 17573564]