
Introduction
The subclavian artery serves as the major blood supply to the upper extremities. It also supplies parts of the head, neck, and thorax. One of the thoracic branches of the subclavian artery is the thyrocervical trunk (TCT).[1]
The thyrocervical trunk is an important vascular supply, as it yields arteries to numerous structures such as organs of the neck, muscles, and the brachial plexus. All this occurs in the tight space of the neck. Therefore, the thyrocervical trunk and its branches have an intricate interplay with the other structures found in their vicinity, which leads to several considerations of surgical and practical relevance. This review aims to confer a thorough understanding of this structure’s anatomy along with shedding light on clinical applications.[2]
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The thyrocervical trunk is near the medial aspect of the anterior scalene muscles in the supraclavicular triangle. The thyrocervical trunk ascends vertically on each side of the neck and yields four branches. The first branch is the inferior thyroid artery (ITA), which is also the largest branch of the thyrocervical trunk. The ITA traverses the vertebral artery anteriorly and the common carotid artery and internal jugular vein posteriorly to reach the posterior part of the thyroid gland. Inside the thyroid, the ITA anastomoses with the ipsilateral superior thyroid artery and the contralateral ITA. The second branch of the thyrocervical trunk is the ascending cervical artery (ACA). The ACA ascends towards the cervical vertebrae posterior to the internal jugular vein, with the phrenic nerve accompanying the ACA laterally. This artery supplies posterior structures, including parts of the spinal cord and its surrounding meninges, vertebral bodies, and prevertebral muscles. It shares anastomoses with the vertebral artery, the occipital artery, and the ascending pharyngeal artery. The third branch of the thyrocervical trunk is the suprascapular artery (SSA). This branch courses towards the shoulder along the clavicle posteriorly and supplies the rotator cuff muscles and posterior scapular muscles. The SSA is part of a rich anastomosis surrounding the scapula. This anastomosis is termed the scapular anastomosis and is comprised of several arteries along with the SSA: the transverse cervical artery, the dorsal scapular artery, branches of the subscapular artery, and branches of the thoracic aorta. The fourth and final branch of the thyrocervical trunk is the transverse cervical artery (TCA). The TCA ascends to the levator scapula accompanied by the accessory nerve and then divides to the superficial and deep branches of the TCA. The superficial branch of the TCA supplies the superficial posterior neck musculature, and the deep branch supplies the superficial muscles of the back.[2][3]
Embryology
Angiogenic precursors stem from embryonic mesoderm tissue.[4]
We can find the right side subclavian artery (SCA) during intrauterine life (seventh week); this comes from the small tract of the dorsal aorta, from the seventh intersegmental artery of the right side and the fourth aortic artery of the right portion. The left SCA derives from the seventh intersegmental artery of the left portion. Around the seventh week, in the cervical tract, the dorsal intersegmental arterial branches, right and left, form different anastomotic unions, creating the longitudinal channels. The latter forms the various branches of the SCA, such as the supreme intercostal artery, the internal thoracic artery, the vertebral artery, the ascending cervical artery, the transverse cervical artery. The thyrocervical trunk derives from the union of the suprascapular artery, the transverse cervical artery, the ascending cervical artery, and the inferior thyroid artery.
Nerves
The inferior thyroid artery is involved in the path of the recurrent laryngeal nerve, which travels over the artery.
Muscles
The scalene muscles (anterior, middle, and posterior scalenes) play a role in neck posturing and movement as well as breathing due to pulling on the ribs. The middle and posterior scalene muscles receive their blood supply from the ACA and the superficial branch of the TCA.[5]
The trapezius receives its blood supply from the TCA. The trapezius controls scapular motion (elevation, depression, retraction). A useful mnemonic is to remember that the TRAnsverse cervical artery supplies the TRApezius muscles.
The four rotator cuff muscles are the supraspinatus, the infraspinatus, the teres minor, and the subscapularis (rotator cuff acronym: SITS). They control the movement of the shoulder. The main blood supply of the rotator cuff muscles stems from the SSA and the subscapular artery. The SSA is a branch of the thyrocervical trunk and the subscapular artery branches from the axillary artery.[6]
Physiologic Variants
One of the branches of the subclavian artery is the dorsal scapular artery. However, the latter can be a branch of the TCA. Also, the thyrocervical trunk has several possible variations. The most common variation is a short trunk from which the superficial portion of the TSA and the SSA arise. In this variation, the ITA branches from the thyrocervical trunk before the short trunk, but the deep branch of the TCA arises directly from the subclavian artery and not the thyrocervical trunk. The term for this variation is a type I configuration. The second and third most common variations are known as type II and III configurations, respectively. Other variants include branches of the thyrocervical trunk originating directly from the subclavian artery. Furthermore, the SSA can emerge from the subscapular artery instead of being a branch of the thyrocervical trunk.[2][7]
Surgical Considerations
Surgery in the head and neck region necessitates knowledge of the intricate anatomy of the region involved. Additionally, the surgeon needs to keep in mind the possible anatomical variations that exist. The surgeon must consider the potential aberrant origin of branches. For detailed vascular imaging, computed tomography angiography (CT) is most commonly employed.[7]
Thyroidectomy can be complicated by bleeding due to an injury of the ITA. In such cases, ligation of the proximal ITA can mitigate the bleeding.
From a surgical point of view, the thyrocervical trunk merits consideration as an area of interest for neurologists and angiologists. The thyrocervical trunk can be involved for endovascular procedures such as embolizations (embolization is an interventional radiology intervention, which involves selective occlusion of some blood vessels); paragangliomas or glomus tumors (benign tumors that originate from some corpuscles responsible for controlling blood pressure distributed along the course of some nerves at the level of the middle ear and the cranial base); cervical vertebral metastasis; hemangioblastoma (rare, benign, highly vascularized tumor of the central nervous system, most commonly located in the cerebellum or spinal cord, onset in adulthood, or other non-cerebral sites); aneurysms; vertebral aneurysmal bone cyst (is a bone hamartoma (malformation) which consists of reactive hemorrhagic tissue that grows inside a bone).
Clinical Significance
The scapular anastomosis provides a rich blood supply to the muscles of the back and shoulders. This ensures adequate circulation even in the event of the occlusion of one of the branches involved in the anastomosis. This fact is especially evident in the event of a gradual occlusion; blood can still reach the target organ via the collateral blood supply, and symptoms might not be present.
An aneurysm or pseudoaneurysm might develop in the thyrocervical trunk. Dysphagia due to compression of the esophagus might ensue. The physical exam may be normal or might reveal a neck mass. Diagnosis is made or confirmed via computed tomography.
Injury to the thyrocervical trunk or its branches can occur due to trauma or iatrogenic injury. One example of iatrogenic injury is during cardiac interventions. Percutaneous coronary intervention is usually via trans-radial artery access. A rare yet devastating complication is thyrocervical trunk perforation. Prompt recognition and treatment are essential since the perforation can lead to a neck hematoma that compresses the trachea and thus compromises the airway.
Tumors in the head and neck can receive blood supply from the thyrocervical trunk or one of its branches. Treatment of such tumors can involve the embolization of the culprit branches. A solid understanding of the anatomy of the thyrocervical trunk enables employing adequate vascular treatment as well as recognizing symptoms of complications.[8][9]
Other Issues
Caution is necessary when reading about the arteries of the neck, as resources might use the same name in different contexts. For example, the transverse cervical artery is sometimes used in more than one meaning. The date and location of publications should be taken into account when interpreting such literature.[1]
Media
(Click Image to Enlarge)
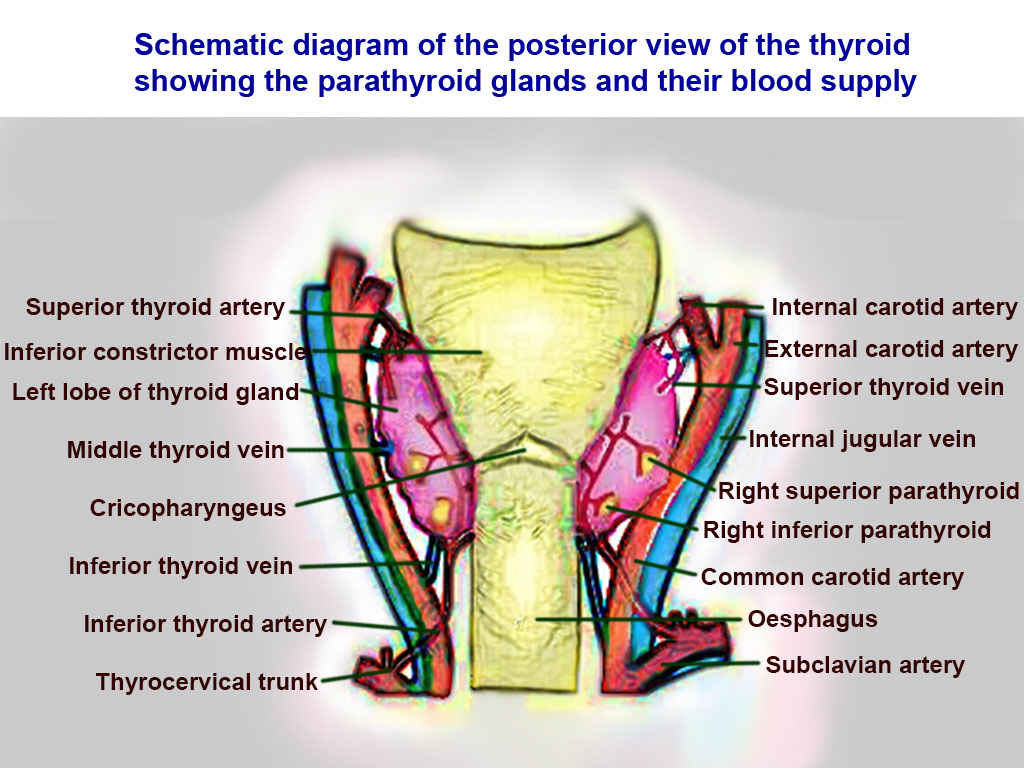
Thyroid Arteries, Veins, and Muscles. Posterior view of thyroid includes superior thyroid, inferior constrictor, left lobe of thyroid, middle thyroid vein, cricopharyngeaus, inferior thyroid vein, inferior thyroid vein, inferior thyroid artery, thyrocervical trunk, internal carotid, external carotid, superior thyroid, internal jugular, right superior parathyroid, right inferior parathyroid, common carotid, oesphagus, and subclavian.
Contributed by T Silappathikaram
(Click Image to Enlarge)

Superficial Arteries of the Chest and Abdomen; Right side, Musculophrenic Artery, Scalenus Anterior, Thyrocervical Artery, Common Carotid Artery, Innominate Artery, Internal Mammary Artery, Perforating Branches, Superior Epigastric Artery, Inferior Epigastric Artery, External Iliac Artery
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
References
Weiglein AH, Moriggl B, Schalk C, Künzel KH, Müller U. Arteries in the posterior cervical triangle in man. Clinical anatomy (New York, N.Y.). 2005 Nov:18(8):553-7 [PubMed PMID: 16187318]
Pérez-García C, Malfaz C, Del Valle Diéguez M, Fortea Gil F, Saura Lorente J, Echenagusia Boyra M, González Leyte M, Pérez-Higueras A, Castro-Reyes E. Embolization through the thyrocervical trunk: vascular anatomy, variants, and a case series. Journal of neurointerventional surgery. 2018 Oct:10(10):1012-1018. doi: 10.1136/neurintsurg-2018-013808. Epub 2018 Mar 29 [PubMed PMID: 29599183]
Level 2 (mid-level) evidenceLischka MF, Krammer EB, Rath T, Riedl M, Ellböck E. The human thyrocervical trunk: configuration and variability reinvestigated. Anatomy and embryology. 1982:163(4):389-401 [PubMed PMID: 7091707]
Noden DM. Embryonic origins and assembly of blood vessels. The American review of respiratory disease. 1989 Oct:140(4):1097-103 [PubMed PMID: 2478056]
Level 3 (low-level) evidenceBordoni B, Varacallo M. Anatomy, Head and Neck, Scalenus Muscle. StatPearls. 2023 Jan:(): [PubMed PMID: 30085600]
McCausland C, Sawyer E, Eovaldi BJ, Varacallo M. Anatomy, Shoulder and Upper Limb, Shoulder Muscles. StatPearls. 2023 Jan:(): [PubMed PMID: 30521257]
Alexander JG, Silva Baptista JD. Coexistence of a rare case of a suprascapular artery with other vascular abnormalities: case report and potential surgical relevance. Surgical and radiologic anatomy : SRA. 2020 Mar:42(3):239-242. doi: 10.1007/s00276-019-02401-w. Epub 2020 Jan 2 [PubMed PMID: 31897655]
Level 3 (low-level) evidenceGhori MA, Al Zubaidi A, Khwaja A. Thyrocervical trunk perforation: A rare vascular complication during cardiac intervention through right radial approach: A case report and literature review. Journal of the Saudi Heart Association. 2019 Jul:31(3):121-124. doi: 10.1016/j.jsha.2019.03.002. Epub 2019 Mar 28 [PubMed PMID: 31031551]
Level 3 (low-level) evidenceMur TA, Anis MM, Soliman AM. Thyrocervical trunk pseudoaneurysm presenting as a neck mass. Ear, nose, & throat journal. 2017 Jul:96(7):238-239 [PubMed PMID: 28719704]