Introduction
The cardiac conduction system is formed by specialized fibers that initiate electrical impulse and conduct it through the heart's chambers. The human heart's dominant pacemaker is the sinus node, which generates an impulse to depolarize the atria and ventricles. The impulse the sinus node generates spreads to the atria and atrial depolarization, or contraction, occurs. This action is marked by the P wave on a surface electrocardiogram (ECG). After atrial depolarization, the wave of depolarization transfers to the ventricles via the atrioventricular (AV) conduction system. QRS marks ventricular depolarization on a surface ECG.[1]
The AV conduction system consists of an AV node and specialized conduction fibers forming the His-Purkinjie system.[2] The autonomic nervous system supplies the AV conduction system, particularly the AV node, resulting in variable conduction during various physiological states.[3] AV conduction is evaluated by assessing the relationship between the P waves and QRS complexes. Typically, a P wave precedes each QRS complex by a fixed PR interval of 120 to 200 milliseconds.[4] An AV block represents a delay or disturbance in the transmission of an impulse from the atria to the ventricles. This can be due to an anatomical or functional impairment in the heart's conduction system.[5] An AV block can manifest as either temporary or permanent, and its severity determines its classification into three types: first-degree, second-degree, and third-degree AV block. Anatomically, an AV block is classified as either a supra (nodal) or intra/infra-His (infranodal) block.[6] Infranodal blocks commonly present with a wide QRS complex, progress to the third-degree AV block, and require pacemakers.[7]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
An AV block could be congenital or acquired. Congenital AV block can be associated with congenital heart diseases, including AV canal defects, transposition of great arteries, heterotaxy syndrome, left atrial isomerism, and tetralogy of Fallot.[8][9] Congenital AV block without structural heart disease, is relatively more common than those associated with congenital heart disease. Immune-mediated conduction system dysfunction is the main reason for congenital AV block in patients without congenital heart disease.[10] Systemic lupus erythematosus is one of the common autoimmune diseases associated with congenital AV block.[11] Maternal viral infection is another cause of congenital AV block in offspring.[12]
Myocardial ischemia/infarction, drugs, electrolyte abnormalities, endocrine disorders, and toxins cause acquired AV block. However, age-related degeneration of conduction system diseases is the most common cause of acquired AV block.[13] About half of such cases result from chronic idiopathic fibrosis and sclerosis of the conduction system, as seen in Lenègre disease and Lev disease.[14][15] Higher vagal tone also causes AV block, especially in young individuals. The vagally mediated AV block is nodal in origin; it is benign and rarely requires pacemaker implantation.[16] Some atrial cardiomyopathies and muscular dystrophies also lead to bradyarrhythmias and AV blocks.[17][18]
The other causes of acquired AV block include infiltrative cardiomyopathies, myocarditis, Lyme disease, rheumatic fever, and endocarditis. Cardiac surgery is also a risk factor for developing an AV block, and aortic and valve surgeries are commonly associated with an AV block due to its proximity to the conduction system.[19] Transcatheter aortic valve replacement is also found to be associated with an AV block. Male patients have a higher incidence of an AV block after transcatheter aortic valve replacement, especially in the presence of underlying conduction system diseases.[20]
Epidemiology
The precise prevalence of AV blocks remains unknown due to the absence of extensive population-based studies focusing specifically on their occurrence. The estimated occurrence of autoantibody-mediated congenital AV block is approximately 1 in 15,000 births. However, it is important to note that the actual incidence may be underestimated due to cases resulting in intrauterine deaths.[21] An AV block due to degeneration of cardiac conduction tissue is much more common in individuals older than 65. In contrast, the prevalence of third-degree AV block is rare in young individuals.[13] However, one study suggested that first-degree AV block is more prevalent in African-American patients than Caucasian patients in all age groups except in the eighth decade of life.[22] However, at this time, there is no well-characterized large study about the correlation between different types of AV block with age, race, or gender.
Pathophysiology
Congenital AV block mediated by the immune system results from the transfer of maternal antibodies (anti-Ro and anti-La) across the placenta into the fetal circulation. These antibodies bind to fetal myocytes and impair cytoplasmic calcium metabolism leading to apoptotic cell death in the conduction system tissues.[10] The result of this immune-mediated process is the fibrosis of the cardiac conduction system and surrounding myocardium.[23] The presence of congenital AV block in individuals with congenital structural heart diseases can be attributed to abnormal development of the central fibrous body and abnormal development or disruption of the AV conduction tissue.[8]
Acquired AV block in older individuals is characterized by degeneration and fibrosis of the His-Purkinje system. Age-related degeneration is a chronic process commonly involving the intra/infra-His conduction system, and most patients require pacemaker implantation.[24] AV blocks occurring after cardiac surgery and transcatheter aortic valve replacement are primarily caused by the mechanical effects exerted on the surrounding conduction system.[19][25]
Toxicokinetics
The following medications can affect AV conduction and may cause an AV block, especially in the presence of underlying conduction system disease.[26][27]
- Digoxin
- Nondihydropyridin calcium channel blockers
- Beta blocking drugs
- Adenosine
- Class I and Class III antiarrhythmic drugs
- Donepezil
- Lithium
History and Physical
History
History taking for patients with concerns for an AV block should include: [28]
- History of heart disease, both congenital and acquired
- Complete list of medications and dosing. Particular drugs of interest include beta-blockers, calcium channel blockers, antiarrhythmic drugs, digoxin
- Recent cardiac procedure
- Signs and symptoms associated with other systemic diseases associated with heart block (amyloidosis, sarcoidosis)
- Baseline exercise capacity
- Potential exposure to tick bites
Patients with first and Mobitz type I, second-degree AV blocks are usually asymptomatic and diagnosed incidentally on examination or a 12-lead ECG. Patients with an AV block commonly present with symptoms such as dyspnea on exertion, easy fatigability, dizziness, and syncope. However, it is rare for them to exhibit cardiac arrest or experience sudden cardiac death.[29]
Physical Exam
Although a physical exam has a limited role in diagnosing an AV block, it is essential to assess underlying structural heart diseases and evaluate the hemodynamic consequences of an AV block.[30] Physical examination findings in cases of an AV block typically include bradycardia, an irregular pulse, hypotension, and the presence of distended neck veins characterized by prominent A waves.[31]
Evaluation
Classification of Atrioventricular Block
First-degree Atrioventricular Block. First-degree AV block is a 1:1 association between P waves and QRS (1:1 AV conduction) and a constant PR interval of >200 ms. The condition is more accurately defined as an AV delay because no P waves are blocked.[32] In the first-degree AV block, the P waves always precede the QRS complexes, but the PR interval is prolonged without any dropped beats. (Figure.1) In other words, while the impulse is slowed, it can still reach the ventricles. The delay is typically due to a minor AV conduction defect occurring at or below the AV node. If the PR interval is more than 300 milliseconds, it is considered a “marked” first-degree AV block, and the P waves may be buried in the preceding T wave.[33]
Second-degree Atrioventricular Block. Second-degree or incomplete AV block occurs when there is intermittent AV conduction. Second-degree AV blocks can be further classified into Mobitz type 1 (Wenckebach) or Mobitz type 2, which can be distinguished by examining the PR interval.
- Second degree, Mobitz type I (Wenckebach). AV block is characterized by P waves exhibiting a consistent rate (<100 bpm) and a gradual prolongation of the PR interval. This is followed by periodic occurrences of single non-conducted P waves, typically accompanied by P waves preceding and following the non-conducted P waves. (Figure.2) Wenckebach is a phenomenon commonly associated with the AV nodes; however, there are reported cases of Wenckebach associated with infra-nodal AV block.[34]
- Second degree, Mobitz type II. AV block is characterized by P waves occurring at a constant rate (<100 bpm) and periodic single non-conducted P waves that arise at unpredictable intervals. These non-conducted P waves are typically observed alongside other P waves, both before and after the non-conducted P wave, and exhibit consistent PR intervals.[35] Conduction of at least two consecutive P waves is required to differentiate Wenckebah from Mobitz type 2 AV block. (Figure.3) When every other P wave is blocked (not conducted), it is impossible to differentiate between Wenckebach and Mobitz type II AV block, so this entity is called a 2:1 AV block.[36]
- Second degree, high-grade. Advanced (high-grade) AV block is defined as the presence of ≥2 consecutive, non-conducted P waves occurring at a constant physiologic rate, along with evidence of AV conduction (manifesting as AV association). (Figure.4)
Third-degree (complete). AV conduction is absent in third-degree or complete heart block, and the P waves are never related to the QRS complexes. In other words, the supraventricular impulses generated do not conduct to the ventricles. Instead, if ventricular conduction occurs, it is maintained by a junctional or ventricular escape rhythm.[29] There is a complete dissociation between the atria and ventricles. The atria and ventricles conduct independently of each other. The P waves (atrial activity) are said to “march through” the QRS complexes at their regular, faster rate. The QRS complexes (ventricular activity) also occur at a regular but slower rate. Two independent rhythms occur simultaneously. (Figure.5)
Evaluation of Patients with Atrioventricular Block
Non-Invasive Evaluation. A resting 12 lead ECG is essential for evaluating patients with a suspected AV block. It helps assess the severity of an AV block, localize the site of the AV block, and provide information about the associated structural heart diseases. However, a 12-lead ECG may not always provide a direct correlation between the observed symptoms and the presence of an AV block.[37] Ambulatory ECG monitoring is considered a superior diagnostic tool to establish a more accurate correlation between symptoms and an AV block. It offers a higher diagnostic yield for identifying a paroxysmal AV block, thereby aiding in the accurate diagnosis of this condition.[38] An exercise ECG may be considered in selective individuals to assess the exercise-induced AV block and localize the site of the block in patients with 2:1 AV block.[39]
Echocardiogram is recommended in every patient with an AV block to exclude structural heart diseases. Cardiac magnetic resonance imaging (cMRI) can be considered in selective individuals suspected of AV blocks due to myocarditis or infiltrative cardiomyopathies.[40] Screening and testing for sleep apnea are recommended in patients with sleep-related AV block to provide proper treatment.
Invasive Evaluation: Routine invasive evaluation is not recommended for an AV block. In cases where initial non-invasive investigations fail to provide a definitive diagnosis, patients experiencing symptoms related to bradycardia should be considered for an implantable loop recorder or an electrophysiology study.[41][42]
Laboratory Investigations: Selected laboratory investigations, including thyroid function tests, electrolyte levels, renal profile, and digoxin levels, should be checked in patients presenting with an AV block if indicated based on clinical evaluation. Genetic testing may be considered in patients with inherited AV blocks, followed by cascade screening and genetic counseling.[43]
Treatment / Management
In most cases, asymptomatic patients with first-degree or second-degree Mobitz type 1 atrioventricular block do not necessitate treatment. However, it is crucial to discontinue any medications triggering the AV block and address any reversible factors contributing to its occurrence. Patients can be monitored on an outpatient basis. However, patients with higher degrees of an AV block (Mobitz type 2 AV block, 3rd degree) tend to have severe damage to the conduction system. They are usually at a greater risk of progressing into asystole, ventricular tachycardia, or sudden cardiac death. Hence, they require urgent admission for cardiac monitoring and further evaluation.[26][28](A1)
Use of an urgent or emergent temporary transvenous pacemaker should not be a "knee-jerk" reaction to the presence of a second-degree, high grade or third-degree AV block. It should be carefully considered after evaluating the risk-benefit ratio in clinical settings. Factors such as hemodynamic stability, including the assessment of systolic blood pressure and the severity and duration of the patient's clinical symptoms, should be considered. Additionally, the level of an AV block and the presence of an appropriate escape rhythm should be considered before making a decision.[44]
Acute Management of Atrioventricular Block
Patients with suspected reversible causes of an AV block, such as digoxin toxicity, Lyme myocarditis, or an overdose of AV node-blocking drugs, often require medical therapy. This may involve administering specific reversal agents or targeted treatments to address the underlying cause and restore normal AV conduction. Intravenous atropine should be considered as initial therapy when the AV block is suspected to be supra-Hisian. Dopamine and isoproterenol can be used in symptomatic patients with second or third-degree AV block with evidence of acute myocardial ischemia.[45] (B2)
A temporary transvenous pacemaker should be considered in selective patients with hemodynamically unstable AV block who do not respond to medical therapy or are in cardiogenic shock.[46][47][48] It is important to minimize the use of temporary pacemakers, particularly in patients needing a permanent pacemaker, as they can significantly elevate the risk of infection associated with cardiac implantable electronic devices. The use of a temporary pacemaker should be kept to the shortest duration to avoid patients' risk of immobility, infection, thromboembolism, and risk of cardiac perforation. The potential complications must be kept in mind as sometimes the risk-benefit ratio may significantly outweigh justifying its potential use.(B2)
Chronic Management of Atrioventricular Block
Implantation of a permanent pacemaker is the mainstay of treatment for patients with AV block. Asymptomatic patients with first-degree AV block, second-degree type I AV block, or 2:1 AV block at the AV node level usually do not require a pacemaker. They should be followed as an outpatient, and a pacemaker should be considered if they develop symptoms due to an AV block.[49][50] Permanent pacemaker implantation must be considered in patients with symptomatic second-degree AV block, high-degree AV block, or third-degree AV block who do not have a reversible cause of the AV block. Patients who exhibit second-degree or third-degree atrioventricular (AV) block and have conditions such as infiltrative cardiomyopathy or muscular dystrophy should receive both a defibrillator and a permanent pacemaker implantation.[49][51][52] According to the current guidelines, a dual-chamber pacemaker is recommended over a single-chamber pacemaker. Nevertheless, a single-chamber pacemaker may be considered in specific cases with persistent atrial fibrillation or significant co-morbid conditions that restrict the advantages of a dual-chamber pacemaker.[53][54](A1)
Differential Diagnosis
All patients presenting with an AV block must undergo extensive work-up to evaluate the underlying causes of the AV block. A 12-lead ECG should be examined closely to differentiate an AV block from an isorhythmic AV dissociation and a junctional escape rhythm.[55]
Prognosis
Atrioventricular block is the most common indication of pacemaker implantation worldwide. Untreated patients diagnosed with third-degree AV block face a 5-year survival rate as low as 37%. Asymptomatic patients with an AV block have a slightly better prognosis than symptomatic patients. Men diagnosed with a third-degree AV block generally exhibit poorer prognoses than women.[56] The prognosis of these patients also depends on the patient's age and the presence of medical conditions such as hypertension, ischemic heart disease, diabetes mellitus, chronic kidney disease, and underlying heart disease.[57] Implantation of pacemakers improves survival and quality of life in symptomatic patients with an AV block.[58][59]
Complications
The common complications of an AV block include syncope, heart failure, atrial fibrillation, and cardiac arrest. It may also lead to bradycardia-induced ventricular tachycardia and rarely may lead to sudden cardiac death.[60]
Deterrence and Patient Education
Patients with first-degree and asymptomatic Mobitz type 1 AV block usually can continue their usual activities but should be advised to avoid medications that can prolong PR interval. Patients diagnosed with Mobitz type 2 and third-degree AV block should have a thorough discussion with their cardiologists regarding the necessity of pacemaker implantation. Furthermore, educating all patients about the alarming symptoms of hypoperfusion, including fatigue, lightheadedness, syncope, presyncope, or angina, is essential. Patients should be informed about the significance of seeking prompt medical attention if they experience these symptoms.
Enhancing Healthcare Team Outcomes
The optimal management of heart block requires an interprofessional team approach, as the condition can lead to significant morbidity and mortality if higher degrees of heart block are missed in the diagnosis. Therefore, collaborative efforts among healthcare professionals are crucial to ensure timely and accurate diagnosis, appropriate treatment, and ongoing monitoring for patients with heart block.
Advanced practice practitioners, primary care providers, internists, or emergency department physicians are among the healthcare professionals who may come across patients presenting with a heart block. Except for first-degree heart block, patients with other types of heart block should be referred to a cardiologist for a more comprehensive and definitive evaluation. In some instances, patients with an AV block may necessitate the implantation of a pacemaker, which can be a life-saving intervention. Post-treatment, it is essential for the cardiology nurse to deliver diligent follow-up care, overseeing the normalization of the patient's heart rate and confirming the absence of any related symptoms.[61]
If patients with a pacemaker require surgery, it is imperative to consult with the cardiologist first. Collaboration with the cardiologist ensures a thorough understanding of the patient's pacemaker settings which may need to be reprogrammed for the procedure, any necessary precautions, and the development of a comprehensive plan to manage the pacemaker during the surgical procedure. After surgery, the pacemaker has to be reprogrammed according to the baseline settings. Today, most centers have a pacemaker nurse who monitors these patients for complications. Only through a combined team approach can the morbidity of heart block be decreased.
Media
(Click Image to Enlarge)
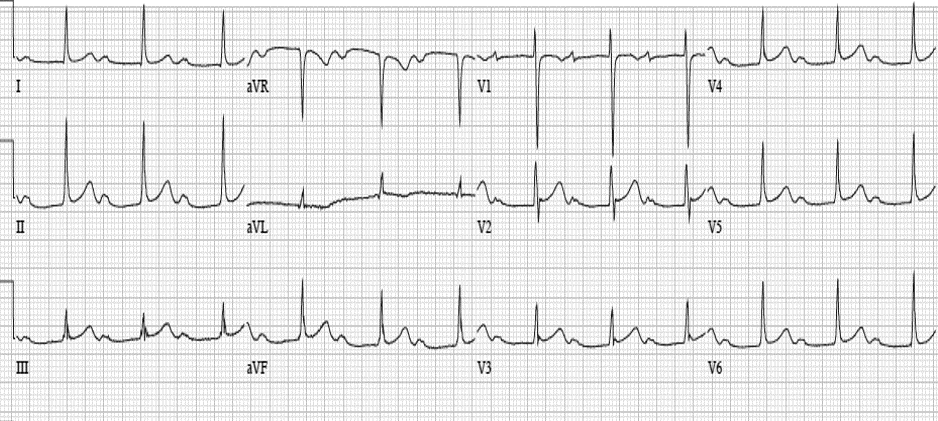
Figure.1. A 12-lead ECG shows constant, prolong PR interval (>200 milliseconds) with 1:1 association of P and QRS, consistent with first degree atrioventricular block. Contributed by Intisar Ahmed
(Click Image to Enlarge)
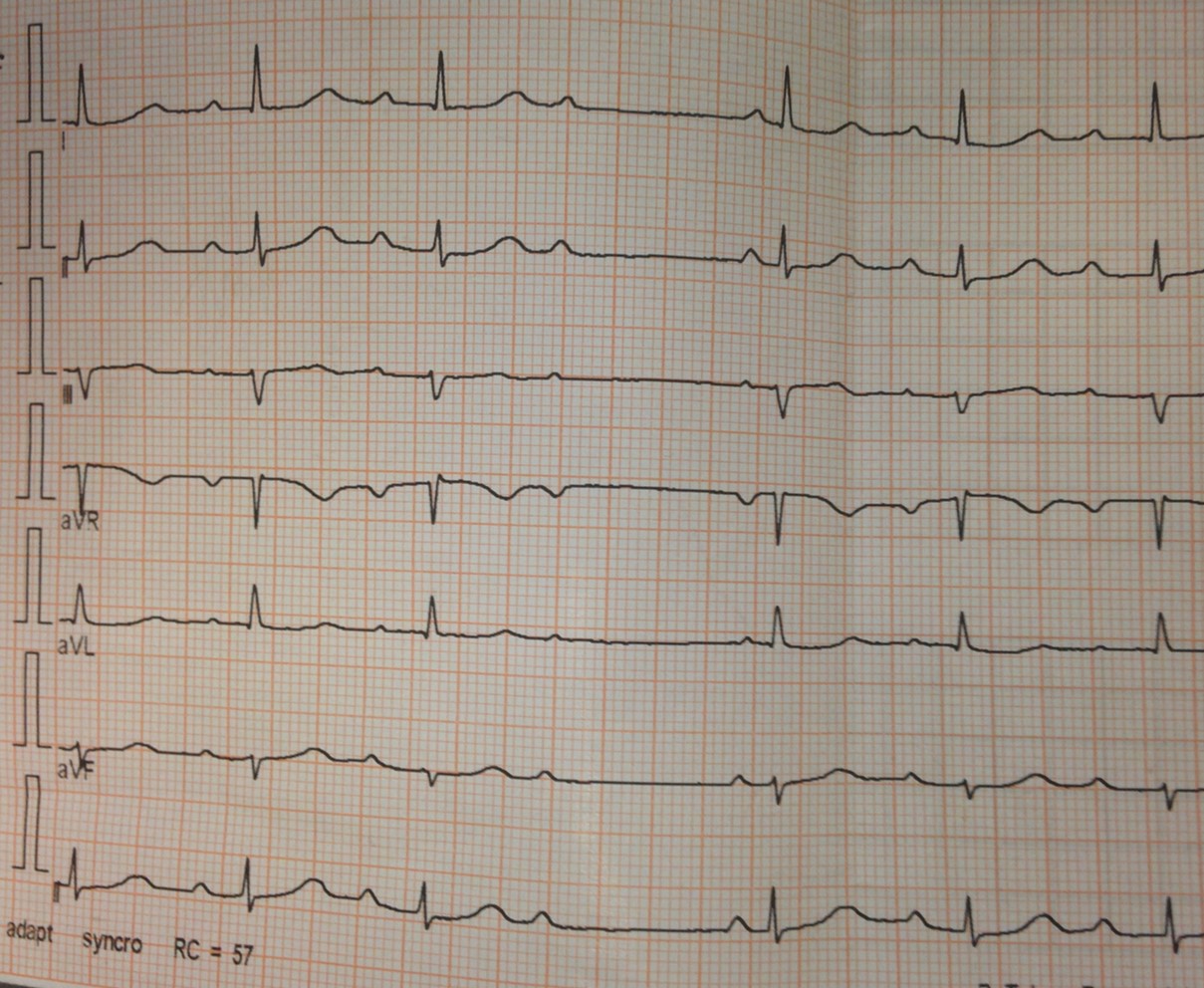
Figure.2. An electrocardiogram shows progressive prolonging of PR interval followed by one blocked P wave, suggestive of second degree type I atrioventricular block (Wenckebach). Contributed by Intisar Ahmed
(Click Image to Enlarge)
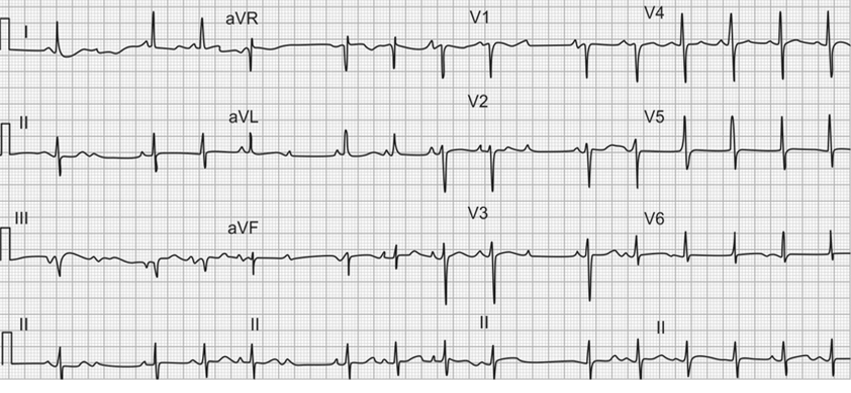
Figure.3. A 12-lead electrocardiogram shows constant PR interval of conducted P waves and a blocked P wave, happening at an unpredictable interval. These findings are consistent with Mobitz type II atrioventricular block. Contributed by Intisar Ahmed
(Click Image to Enlarge)
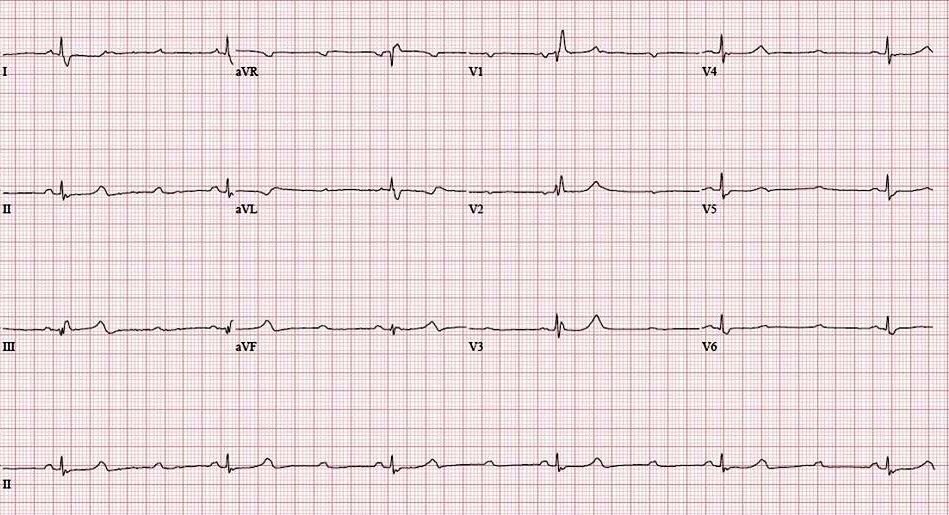
Figure.4. A 12--lead ECG shows two consecutive blocked P waves followed by one conducted P wave, suggestive of high-grade atrioventricular block. Contributed by Intisar Ahmed
(Click Image to Enlarge)
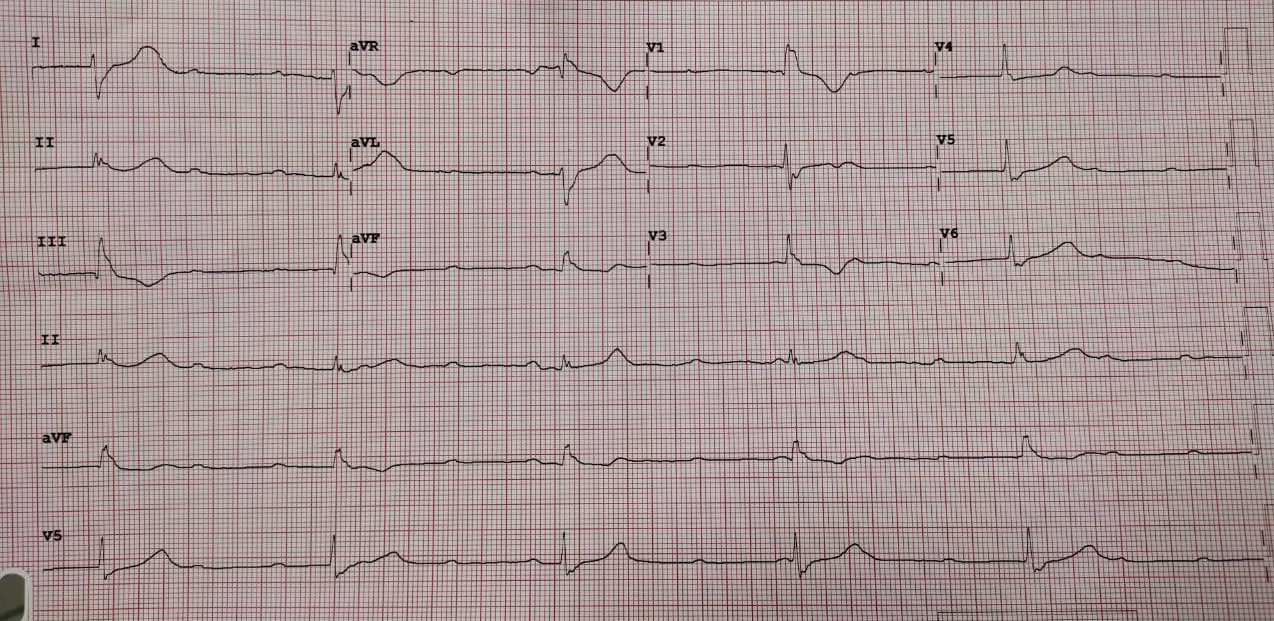
Figure.5. A 12-lead ECG shows P waves at a constant rate with no association of P and QRS complexes and the rate of QRS complex is slower than that of P waves. These findings are suggestive of third degree atrioventricular block. Contributed by Intisar Ahmed
References
Żuchowski B, Błaszyk K, Piskorski J, Wykrętowicz A, Guzik P. Dependence of the Atrioventricular Conduction Time on the Conduction through the Atrioventricular Node and His-Purkinje System. Journal of clinical medicine. 2023 Feb 7:12(4):. doi: 10.3390/jcm12041330. Epub 2023 Feb 7 [PubMed PMID: 36835864]
Wu J, Zipes DP. Mechanisms underlying atrioventricular nodal conduction and the reentrant circuit of atrioventricular nodal reentrant tachycardia using optical mapping. Journal of cardiovascular electrophysiology. 2002 Aug:13(8):831-4 [PubMed PMID: 12212708]
Prystowsky EN, Jackman WM, Rinkenberger RL, Heger JJ, Zipes DP. Effect of autonomic blockade on ventricular refractoriness and atrioventricular nodal conduction in humans. Evidence supporting a direct cholinergic action on ventricular muscle refractoriness. Circulation research. 1981 Aug:49(2):511-8 [PubMed PMID: 7249285]
Kwok CS, Rashid M, Beynon R, Barker D, Patwala A, Morley-Davies A, Satchithananda D, Nolan J, Myint PK, Buchan I, Loke YK, Mamas MA. Prolonged PR interval, first-degree heart block and adverse cardiovascular outcomes: a systematic review and meta-analysis. Heart (British Cardiac Society). 2016 May:102(9):672-80. doi: 10.1136/heartjnl-2015-308956. Epub 2016 Feb 15 [PubMed PMID: 26879241]
Level 1 (high-level) evidenceEpstein AE, DiMarco JP, Ellenbogen KA, Estes NA 3rd, Freedman RA, Gettes LS, Gillinov AM, Gregoratos G, Hammill SC, Hayes DL, Hlatky MA, Newby LK, Page RL, Schoenfeld MH, Silka MJ, Stevenson LW, Sweeney MO, Smith SC Jr, Jacobs AK, Adams CD, Anderson JL, Buller CE, Creager MA, Ettinger SM, Faxon DP, Halperin JL, Hiratzka LF, Hunt SA, Krumholz HM, Kushner FG, Lytle BW, Nishimura RA, Ornato JP, Page RL, Riegel B, Tarkington LG, Yancy CW, American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the ACC/AHA/NASPE 2002 Guideline Update for Implantation of Cardiac Pacemakers and Antiarrhythmia Devices), American Association for Thoracic Surgery, Society of Thoracic Surgeons. ACC/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the ACC/AHA/NASPE 2002 Guideline Update for Implantation of Cardiac Pacemakers and Antiarrhythmia Devices) developed in collaboration with the American Association for Thoracic Surgery and Society of Thoracic Surgeons. Journal of the American College of Cardiology. 2008 May 27:51(21):e1-62. doi: 10.1016/j.jacc.2008.02.032. Epub [PubMed PMID: 18498951]
Level 1 (high-level) evidenceSheldon RS, Lei LY, Solbiati M, Chew DS, Raj SR, Costantino G, Morillo C, Sandhu RK. Electrophysiology studies for predicting atrioventricular block in patients with syncope: A systematic review and meta-analysis. Heart rhythm. 2021 Aug:18(8):1310-1317. doi: 10.1016/j.hrthm.2021.04.010. Epub 2021 Apr 20 [PubMed PMID: 33887450]
Level 1 (high-level) evidenceDhingra RC, Amat-y-Leon F, Pouget JM, Rosen KM. Infranodal block: diagnosis, clinical significance, and management. The Medical clinics of North America. 1976 Jan:60(1):175-92 [PubMed PMID: 1107691]
Warnes CA. Transposition of the great arteries. Circulation. 2006 Dec 12:114(24):2699-709 [PubMed PMID: 17159076]
Karpawich PP, Gillette PC, Garson A Jr, Hesslein PS, Porter CB, McNamara DG. Congenital complete atrioventricular block: clinical and electrophysiologic predictors of need for pacemaker insertion. The American journal of cardiology. 1981 Dec:48(6):1098-102 [PubMed PMID: 7304459]
Ambrosi A, Wahren-Herlenius M. Congenital heart block: evidence for a pathogenic role of maternal autoantibodies. Arthritis research & therapy. 2012 Apr 26:14(2):208. doi: 10.1186/ar3787. Epub 2012 Apr 26 [PubMed PMID: 22546326]
Level 3 (low-level) evidenceBuyon JP, Hiebert R, Copel J, Craft J, Friedman D, Katholi M, Lee LA, Provost TT, Reichlin M, Rider L, Rupel A, Saleeb S, Weston WL, Skovron ML. Autoimmune-associated congenital heart block: demographics, mortality, morbidity and recurrence rates obtained from a national neonatal lupus registry. Journal of the American College of Cardiology. 1998 Jun:31(7):1658-66 [PubMed PMID: 9626848]
Ye Z, Wang L, Yang T, Chen L, Wang T, Chen L, Zhao L, Zhang S, Zheng Z, Luo L, Qin J. Maternal Viral Infection and Risk of Fetal Congenital Heart Diseases: A Meta-Analysis of Observational Studies. Journal of the American Heart Association. 2019 May 7:8(9):e011264. doi: 10.1161/JAHA.118.011264. Epub [PubMed PMID: 30995883]
Level 1 (high-level) evidenceBarra SN, Providência R, Paiva L, Nascimento J, Marques AL. A review on advanced atrioventricular block in young or middle-aged adults. Pacing and clinical electrophysiology : PACE. 2012 Nov:35(11):1395-405. doi: 10.1111/j.1540-8159.2012.03489.x. Epub 2012 Aug 16 [PubMed PMID: 22897386]
LENEGRE J. ETIOLOGY AND PATHOLOGY OF BILATERAL BUNDLE BRANCH BLOCK IN RELATION TO COMPLETE HEART BLOCK. Progress in cardiovascular diseases. 1964 Mar:6():409-44 [PubMed PMID: 14153648]
LEV M. ANATOMIC BASIS FOR ATRIOVENTRICULAR BLOCK. The American journal of medicine. 1964 Nov:37():742-8 [PubMed PMID: 14237429]
Alboni P, Holz A, Brignole M. Vagally mediated atrioventricular block: pathophysiology and diagnosis. Heart (British Cardiac Society). 2013 Jul:99(13):904-8. doi: 10.1136/heartjnl-2012-303220. Epub 2013 Jan 2 [PubMed PMID: 23286970]
Level 3 (low-level) evidenceKottkamp H. Fibrotic atrial cardiomyopathy: a specific disease/syndrome supplying substrates for atrial fibrillation, atrial tachycardia, sinus node disease, AV node disease, and thromboembolic complications. Journal of cardiovascular electrophysiology. 2012 Jul:23(7):797-9. doi: 10.1111/j.1540-8167.2012.02341.x. Epub 2012 May 3 [PubMed PMID: 22554187]
Level 3 (low-level) evidenceRajdev A, Groh WJ. Arrhythmias in the muscular dystrophies. Cardiac electrophysiology clinics. 2015 Jun:7(2):303-8. doi: 10.1016/j.ccep.2015.03.011. Epub 2015 Mar 29 [PubMed PMID: 26002394]
Ferrari AD, Süssenbach CP, Guaragna JC, Piccoli Jda C, Gazzoni GF, Ferreira DK, Albuquerque LC, Goldani MA. Atrioventricular block in the postoperative period of heart valve surgery: incidence, risk factors and hospital evolution. Revista brasileira de cirurgia cardiovascular : orgao oficial da Sociedade Brasileira de Cirurgia Cardiovascular. 2011 Jul-Sep:26(3):364-72 [PubMed PMID: 22086572]
Level 2 (mid-level) evidenceSiontis GC, Jüni P, Pilgrim T, Stortecky S, Büllesfeld L, Meier B, Wenaweser P, Windecker S. Predictors of permanent pacemaker implantation in patients with severe aortic stenosis undergoing TAVR: a meta-analysis. Journal of the American College of Cardiology. 2014 Jul 15:64(2):129-40. doi: 10.1016/j.jacc.2014.04.033. Epub [PubMed PMID: 25011716]
Level 1 (high-level) evidenceChandler SF, Fynn-Thompson F, Mah DY. Role of cardiac pacing in congenital complete heart block. Expert review of cardiovascular therapy. 2017 Nov:15(11):853-861. doi: 10.1080/14779072.2017.1376655. Epub 2017 Sep 13 [PubMed PMID: 28875729]
Upshaw CB Jr. Comparison of the prevalence of first-degree atrioventricular block in African-American and in Caucasian patients: an electrocardiographic study III. Journal of the National Medical Association. 2004 Jun:96(6):756-60 [PubMed PMID: 15233485]
Moak JP, Barron KS, Hougen TJ, Wiles HB, Balaji S, Sreeram N, Cohen MH, Nordenberg A, Van Hare GF, Friedman RA, Perez M, Cecchin F, Schneider DS, Nehgme RA, Buyon JP. Congenital heart block: development of late-onset cardiomyopathy, a previously underappreciated sequela. Journal of the American College of Cardiology. 2001 Jan:37(1):238-42 [PubMed PMID: 11153745]
Bourke JP. Atrioventricular block and problems with atrioventricular conduction. Clinics in geriatric medicine. 2002 May:18(2):229-51 [PubMed PMID: 12180245]
Abu Rmilah AA, Al-Zu'bi H, Haq IU, Yagmour AH, Jaber SA, Alkurashi AK, Qaisi I, Kowlgi GN, Cha YM, Mulpuru S, DeSimone CV, Deshmukh AJ. Predicting permanent pacemaker implantation following transcatheter aortic valve replacement: A contemporary meta-analysis of 981,168 patients. Heart rhythm O2. 2022 Aug:3(4):385-392. doi: 10.1016/j.hroo.2022.05.001. Epub 2022 May 12 [PubMed PMID: 36097458]
Level 1 (high-level) evidenceWriting Committee Members, Kusumoto FM, Schoenfeld MH, Barrett C, Edgerton JR, Ellenbogen KA, Gold MR, Goldschlager NF, Hamilton RM, Joglar JA, Kim RJ, Lee R, Marine JE, McLeod CJ, Oken KR, Patton KK, Pellegrini CN, Selzman KA, Thompson A, Varosy PD. 2018 ACC/AHA/HRS guideline on the evaluation and management of patients with bradycardia and cardiac conduction delay: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Heart rhythm. 2019 Sep:16(9):e128-e226. doi: 10.1016/j.hrthm.2018.10.037. Epub 2018 Nov 6 [PubMed PMID: 30412778]
Level 1 (high-level) evidenceZeltser D, Justo D, Halkin A, Rosso R, Ish-Shalom M, Hochenberg M, Viskin S. Drug-induced atrioventricular block: prognosis after discontinuation of the culprit drug. Journal of the American College of Cardiology. 2004 Jul 7:44(1):105-8 [PubMed PMID: 15234417]
Glikson M, Nielsen JC, Kronborg MB, Michowitz Y, Auricchio A, Barbash IM, Barrabés JA, Boriani G, Braunschweig F, Brignole M, Burri H, Coats AJS, Deharo JC, Delgado V, Diller GP, Israel CW, Keren A, Knops RE, Kotecha D, Leclercq C, Merkely B, Starck C, Thylén I, Tolosana JM. Corrigendum to: 2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy: Developed by the Task Force on cardiac pacing and cardiac resynchronization therapy of the European Society of Cardiology (ESC): With the special contribution of the European Heart Rhythm Association (EHRA). Europace : European pacing, arrhythmias, and cardiac electrophysiology : journal of the working groups on cardiac pacing, arrhythmias, and cardiac cellular electrophysiology of the European Society of Cardiology. 2022 Apr 5:24(4):699. doi: 10.1093/europace/euac023. Epub [PubMed PMID: 35253863]
Knabben V, Chhabra L, Slane M. Third-Degree Atrioventricular Block. StatPearls. 2024 Jan:(): [PubMed PMID: 31424783]
STACK MF, RADER B, SOBOL BJ, FARBER SJ, EICHNA LW. Cardiovascular hemodynamic functions in complete heart block and the effect of isopropylnorepinephrine. Circulation. 1958 Apr:17(4, Part 1):526-36 [PubMed PMID: 13523763]
Morin DP, Bernard ML. Extreme "cannon A waves" and pulsatile skin color in complete heart block. HeartRhythm case reports. 2017 Oct:3(10):493. doi: 10.1016/j.hrcr.2017.06.012. Epub 2017 Aug 7 [PubMed PMID: 29062706]
Level 3 (low-level) evidenceOldroyd SH, Quintanilla Rodriguez BS, Makaryus AN. First-Degree Heart Block. StatPearls. 2024 Jan:(): [PubMed PMID: 28846254]
Lewalter T, Pürerfellner H, Ungar A, Rieger G, Mangoni L, Duru F, INSIGHT XT study investigators. "First-degree AV block-a benign entity?" Insertable cardiac monitor in patients with 1st-degree AV block reveals presence or progression to higher grade block or bradycardia requiring pacemaker implant. Journal of interventional cardiac electrophysiology : an international journal of arrhythmias and pacing. 2018 Aug:52(3):303-306. doi: 10.1007/s10840-018-0439-7. Epub 2018 Aug 13 [PubMed PMID: 30105427]
Burri H, Zimmermann M. Infranodal Wenckebach conduction block and illustration of the gap phenomenon. HeartRhythm case reports. 2021 Feb:7(2):63-64. doi: 10.1016/j.hrcr.2020.11.005. Epub 2020 Nov 13 [PubMed PMID: 33665102]
Level 3 (low-level) evidenceSurawicz B, Childers R, Deal BJ, Gettes LS, Bailey JJ, Gorgels A, Hancock EW, Josephson M, Kligfield P, Kors JA, Macfarlane P, Mason JW, Mirvis DM, Okin P, Pahlm O, Rautaharju PM, van Herpen G, Wagner GS, Wellens H, American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology, American College of Cardiology Foundation, Heart Rhythm Society. AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram: part III: intraventricular conduction disturbances: a scientific statement from the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society. Endorsed by the International Society for Computerized Electrocardiology. Journal of the American College of Cardiology. 2009 Mar 17:53(11):976-81. doi: 10.1016/j.jacc.2008.12.013. Epub [PubMed PMID: 19281930]
Barold SS. 2:1 Atrioventricular block: order from chaos. The American journal of emergency medicine. 2001 May:19(3):214-7 [PubMed PMID: 11326349]
Linzer M, Yang EH, Estes NA 3rd, Wang P, Vorperian VR, Kapoor WN. Diagnosing syncope. Part 1: Value of history, physical examination, and electrocardiography. Clinical Efficacy Assessment Project of the American College of Physicians. Annals of internal medicine. 1997 Jun 15:126(12):989-96 [PubMed PMID: 9182479]
Level 1 (high-level) evidenceLinzer M, Yang EH, Estes NA 3rd, Wang P, Vorperian VR, Kapoor WN. Diagnosing syncope. Part 2: Unexplained syncope. Clinical Efficacy Assessment Project of the American College of Physicians. Annals of internal medicine. 1997 Jul 1:127(1):76-86 [PubMed PMID: 9214258]
Coplan NL, Morales MC, Romanello P, Wilentz JR, Moses JW. Exercise-related atrioventricular block. Influence of myocardial ischemia. Chest. 1991 Dec:100(6):1728-30 [PubMed PMID: 1959424]
Level 3 (low-level) evidenceFontana M, Pica S, Reant P, Abdel-Gadir A, Treibel TA, Banypersad SM, Maestrini V, Barcella W, Rosmini S, Bulluck H, Sayed RH, Patel K, Mamhood S, Bucciarelli-Ducci C, Whelan CJ, Herrey AS, Lachmann HJ, Wechalekar AD, Manisty CH, Schelbert EB, Kellman P, Gillmore JD, Hawkins PN, Moon JC. Prognostic Value of Late Gadolinium Enhancement Cardiovascular Magnetic Resonance in Cardiac Amyloidosis. Circulation. 2015 Oct 20:132(16):1570-9. doi: 10.1161/CIRCULATIONAHA.115.016567. Epub 2015 Sep 11 [PubMed PMID: 26362631]
Fisher JD. Role of electrophysiologic testing in the diagnosis and treatment of patients with known and suspected bradycardias and tachycardias. Progress in cardiovascular diseases. 1981 Jul-Aug:24(1):25-90 [PubMed PMID: 7019962]
Podoleanu C, DaCosta A, Defaye P, Taieb J, Galley D, Bru P, Maury P, Mabo P, Boveda S, Cellarier G, Anselme F, Kouakam C, Delarche N, Deharo JC, FRESH investigators. Early use of an implantable loop recorder in syncope evaluation: a randomized study in the context of the French healthcare system (FRESH study). Archives of cardiovascular diseases. 2014 Oct:107(10):546-52. doi: 10.1016/j.acvd.2014.05.009. Epub 2014 Sep 16 [PubMed PMID: 25241220]
Level 1 (high-level) evidenceAckerman MJ, Priori SG, Willems S, Berul C, Brugada R, Calkins H, Camm AJ, Ellinor PT, Gollob M, Hamilton R, Hershberger RE, Judge DP, Le Marec H, McKenna WJ, Schulze-Bahr E, Semsarian C, Towbin JA, Watkins H, Wilde A, Wolpert C, Zipes DP. HRS/EHRA expert consensus statement on the state of genetic testing for the channelopathies and cardiomyopathies this document was developed as a partnership between the Heart Rhythm Society (HRS) and the European Heart Rhythm Association (EHRA). Heart rhythm. 2011 Aug:8(8):1308-39. doi: 10.1016/j.hrthm.2011.05.020. Epub [PubMed PMID: 21787999]
Level 3 (low-level) evidenceGlikson M, Nielsen JC, Kronborg MB, Michowitz Y, Auricchio A, Barbash IM, Barrabés JA, Boriani G, Braunschweig F, Brignole M, Burri H, Coats AJS, Deharo JC, Delgado V, Diller GP, Israel CW, Keren A, Knops RE, Kotecha D, Leclercq C, Merkely B, Starck C, Thylén I, Tolosana JM, ESC Scientific Document Group. [2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy Developed by the Task Force on cardiac pacing and cardiac resynchronization therapy of the European Society of Cardiology (ESC) With the special contribution of the European Heart Rhythm Association (EHRA)]. Giornale italiano di cardiologia (2006). 2022 Jul:23(7 Suppl 1):e1-e94. doi: 10.1714/3824.38087. Epub [PubMed PMID: 35771031]
Brady WJ, Swart G, DeBehnke DJ, Ma OJ, Aufderheide TP. The efficacy of atropine in the treatment of hemodynamically unstable bradycardia and atrioventricular block: prehospital and emergency department considerations. Resuscitation. 1999 Jun:41(1):47-55 [PubMed PMID: 10459592]
Level 2 (mid-level) evidenceHickey AR, Wenger TL, Carpenter VP, Tilson HH, Hlatky MA, Furberg CD, Kirkpatrick CH, Strauss HC, Smith TW. Digoxin Immune Fab therapy in the management of digitalis intoxication: safety and efficacy results of an observational surveillance study. Journal of the American College of Cardiology. 1991 Mar 1:17(3):590-8 [PubMed PMID: 1993775]
Level 2 (mid-level) evidenceKennebäck G, Tabrizi F, Lindell P, Nordlander R. High-degree atrioventricular block during anti-arrhythmic drug treatment: use of a pacemaker with a bradycardia-detection algorithm to study the time course after drug withdrawal. Europace : European pacing, arrhythmias, and cardiac electrophysiology : journal of the working groups on cardiac pacing, arrhythmias, and cardiac cellular electrophysiology of the European Society of Cardiology. 2007 Mar:9(3):186-91 [PubMed PMID: 17255148]
Bjørnstad CC, Gjertsen E, Thorup F, Gundersen T, Tobiasson K, Otterstad JE. Temporary cardiac pacemaker treatment in five Norwegian regional hospitals. Scandinavian cardiovascular journal : SCJ. 2012 Jun:46(3):137-43. doi: 10.3109/14017431.2012.672763. Epub 2012 Mar 27 [PubMed PMID: 22390277]
Strasberg B, Amat-Y-Leon F, Dhingra RC, Palileo E, Swiryn S, Bauernfeind R, Wyndham C, Rosen KM. Natural history of chronic second-degree atrioventricular nodal block. Circulation. 1981 May:63(5):1043-9 [PubMed PMID: 7471363]
Barold SS, Indications for permanent cardiac pacing in first-degree AV block: class I, II, or III? Pacing and clinical electrophysiology : PACE. 1996 May; [PubMed PMID: 8734740]
Simon AB, Zloto AE. Atrioventricular block: natural history after permanent ventricular pacing. The American journal of cardiology. 1978 Mar:41(3):500-7 [PubMed PMID: 626128]
Level 2 (mid-level) evidenceBhakta D, Shen C, Kron J, Epstein AE, Pascuzzi RM, Groh WJ. Pacemaker and implantable cardioverter-defibrillator use in a US myotonic dystrophy type 1 population. Journal of cardiovascular electrophysiology. 2011 Dec:22(12):1369-75. doi: 10.1111/j.1540-8167.2011.02200.x. Epub 2011 Oct 28 [PubMed PMID: 22035077]
Connolly SJ, Kerr CR, Gent M, Roberts RS, Yusuf S, Gillis AM, Sami MH, Talajic M, Tang AS, Klein GJ, Lau C, Newman DM. Effects of physiologic pacing versus ventricular pacing on the risk of stroke and death due to cardiovascular causes. Canadian Trial of Physiologic Pacing Investigators. The New England journal of medicine. 2000 May 11:342(19):1385-91 [PubMed PMID: 10805823]
Level 1 (high-level) evidenceSweeney MO, Hellkamp AS, Ellenbogen KA, Greenspon AJ, Freedman RA, Lee KL, Lamas GA, MOde Selection Trial Investigators. Adverse effect of ventricular pacing on heart failure and atrial fibrillation among patients with normal baseline QRS duration in a clinical trial of pacemaker therapy for sinus node dysfunction. Circulation. 2003 Jun 17:107(23):2932-7 [PubMed PMID: 12782566]
SANGHVI LM. Isorhythmic dissociation. The American journal of cardiology. 1961 Aug:8():293-6 [PubMed PMID: 13746248]
Edhag O, Swahn A. Prognosis of patients with complete heart block or arrhythmic syncope who were not treated with artificial pacemakers. A long-term follow-up study of 101 patients. Acta medica Scandinavica. 1976:200(6):457-63 [PubMed PMID: 1015354]
Johansson BW. Complete heart block. A clinical, hemodynamic and pharmacological study in patients with and without an artificial pacemaker. Acta medica Scandinavica. Supplementum. 1966:451():1-127 [PubMed PMID: 5223645]
Lopez-Jimenez F, Goldman L, Orav EJ, Ellenbogen K, Stambler B, Marinchak R, Wilkoff BL, Mangione CM, Yoon C, Vitale K, Lamas GA. Health values before and after pacemaker implantation. American heart journal. 2002 Oct:144(4):687-92 [PubMed PMID: 12360166]
Level 1 (high-level) evidenceEdhag O. Long-term cardiac pacing. Experience of fixed-rate pacing with an endocardial electrode in 260 patients. Acta medica Scandinavica. Supplementum. 1969:502():9-110 [PubMed PMID: 5265649]
Jeon JH, Her SH, Chin JY, Park KH, Yoon HJ, Lee JM, Jin SW. Complete atrioventricular block-induced Torsade de pointes, manifested by epilepsy. The Korean journal of internal medicine. 2011 Mar:26(1):99-102. doi: 10.3904/kjim.2011.26.1.99. Epub 2011 Mar 2 [PubMed PMID: 21437170]
Level 3 (low-level) evidenceIrwin ME. Cardiac pacing device therapy for atrial dysrhythmias: how does it work? AACN clinical issues. 2004 Jul-Sep:15(3):377-90 [PubMed PMID: 15475812]