Introduction
Refractive surgery is a surgical laser procedure to alter the eye's refractive power and decrease the patient's dependence on spectacles and contact lenses. Radial keratotomy (RK) was one of the first and most commonly performed refractive surgical procedures of the 20th century. Approximately 10% of practicing ophthalmologists in the United States have performed several hundred thousand RK procedures.[1] Lans demonstrated that deep radial incisions in the anterior cornea caused central corneal flattening with peripheral steepening in the late 19th century, followed by Sato, who performed posterior RKs in a series of eight keratoconus patients in the 1930s.[1][2] Enhanced flattening was achieved with longer and deeper incisions. Although initially successful, Sato's technique ultimately resulted in bullous keratopathy in up to 70% of patients due to endothelial damage.[3]
Improvements to the technique so that incisions were placed solely on the anterior corneal surface were undertaken in the 1970s in Russia, where the use of multifactorial formulae and nomograms, which incorporated patient and surgical variables, led to improved predictability.[4][5][6] Radial keratotomy correction was introduced to the USA in 1978 by Bores et al., Myers, and Cowden, with multiple surgeons performing and publishing anecdotal results.[7][8][9][10] Early publications were optimistic, and there were few reported complications. This led the National Institutes of Health to fund the Prospective Evaluation of Radial Keratotomy (PERK) study to assess the safety, efficacy, stability, and predictability of RK.[11] The PERK study involved 12 surgeons practicing in nine clinical centers who performed RKs on 793 eyes of 435 patients who had 2.00-8.00 D of myopia.[11] Technique refinements and improvements continued after the PERK study. Younger patients have a greater rate and degree of wound healing, and therefore require more surgery for the same effect compared to older individuals. Better equipment e.g., diamond blades and calibration with ultrasonic pachymeters, further improved predictability.
With the introduction of more accurate and stable laser refractive surgery i.e., photorefractive keratectomy (PRK), Laser In Situ Keratomileusis (LASIK), small incision lenticule extraction (SMILE), and intraocular lens surgery the popularity of radial keratotomy correction has decreased considerably. However, due to the number of patients who have undergone this procedure, knowledge of the procedure and its variations are required to manage this group of patients who may require visual rehabilitation in later life.
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
The eye acts as a compound optical system and comprises a corneal and a lens portion. The total refracting power of the normal eye is approximately 64 D, with the cornea accounting for two-thirds (43 D). The anterior and posterior corneal surfaces and the crystalline lens focus the incident light rays onto the retina. In an emmetropic (normally sighted) eye, light rays from infinity are focused on the retina with the dioptric power equal to the axial length of the eye. Images are therefore in focus. In ametropic eyes, the eye is either too long or short or has astigmatism, and thus the light rays are unable to be brought to a focus on the retina.
The normal cornea is a transparent avascular structure, which is convex in shape. The average diameter measures 11.5 mm, and thickness increases from 550 to 565 μm centrally to 610 to 640 μm peripherally.[12] There is dense innervation supplied by long ciliary nerves originating in the ophthalmic division of the trigeminal nerve.[13] The cornea is made up of different layers, comprising the epithelium, Bowman's layer, stroma, pre-Descemet's layer (Dua's layer), Descemet's layer, and endothelium. The corneal epithelium acts as the main barrier to the eye, and the tear film provides a smooth optical surface. There are five to seven cellular layers in the center, increasing to seven to ten layers in the periphery. The average thickness of the epithelium is 50 μm. When an epithelial defect occurs e.g., corneal abrasion, limbal stem cells proliferate in the periphery and migrate to the area of defect, replacing lost cells.[14] Bowman's layer (anterior limiting lamina) makes up the most anterior aspect of the corneal stroma and comprises 8 to 12 μm of densely formed mainly type I collagen fibrils. Bowman's layer decreases with aging, and histopathological changes have been demonstrated in keratoconus patients.[15]
The corneal stroma provides mechanical strength and consists of collagen fibers, interconnected keratocytes, and glycosaminoglycans in regular and densely packed lamellae. In the central cornea, these lamellae have a higher density anteriorly compared with the posterior. Incisional surgery such as RK will disrupt this layer and decrease the mechanical strength of the cornea permanently.
Descemet's membrane is a basement membrane that measures 5 to 10 μm and is divided into an anterior and a posterior layer. The posterior layer is produced by the endothelial cells and increases in thickness with advancing age.[16] The corneal endothelium is a single layer of cells on the most posterior aspect of the corneal surface. It is responsible for the osmotic balance of the cornea, preventing corneal edema and loss of transparency. The endothelium is non-regenerating, and cell density steadily decreases with age.[17]
Radial keratotomy correction aims to change the refractive power of the anterior corneal surface to correct ametropia by the creation of individual linear incisions deep into the stroma (80 to 90% depth). The number of incisions ranges from 4 to 24, with 8 being the most commonly used.[18] The length, depth, and number of incisions, gender, and age of the patient contribute to the surgical outcome.
Indications
Radial keratotomy correction is indicated for patients with moderate myopia. Patients should be at least 18 years of age because they require stable refraction and be able to provide informed consent for surgery. Contact lens wearers will need to remove the lenses and have several serial corneal topography scans and cycloplegic refractions to ensure refractive stability before proceeding to surgery.
Contraindications
Absolute Contraindications
Contraindications of radial keratotomy are similar to that of other types of refractive surgical correction. Absolute contraindications include refractive instability, defined as changes greater than 0.5 D within the last 12 months. Systemic conditions that can lead to refractive instability include pregnancy and uncontrolled diabetes mellitus. Patients with unstable collagen vascular diseases such as systemic lupus erythematosus, Sjögren's syndrome, Graves' disease, rheumatoid arthritis, inflammatory bowel disease are at risk of having or developing ocular conditions which directly affect vision or cause decreased wound healing, such as keratoconjunctivitis sicca.[19] Cornea ectasia can develop in the cornea post-surgery if the cornea is too mechanically week. Therefore, patients with keratoconus and/or thinner corneas i.e., less than 500 μm centrally, are not suitable for surgery. Patients with active ocular surface infection (keratitis) or inflammation can worsen their conditions by undergoing surgery and are contraindicated from proceeding.
Relative Contraindications
These will vary with the individual patient.
- Patients with advancing age can have cataracts developing, which will adversely affect visual acuity despite RK correction. Cataract surgery with intraocular lens implantation may be a better option for these patients to improve unaided distance visual acuity.
- If there is co-existing corneal pathology, e.g., scarring, corneal dystrophy, and herpetic eye disease, final visual improvement will be harder to achieve with a greater risk of visual loss.
- Patients with larger pupil diameter size may be more affected by postsurgical visual symptoms of glare and haloes, especially in dim light.[20] Normal adult pupil size measures 2 to 4 mm in diameter in bright light to 4 to 8 mm in the dark. Pupil asymmetry of up to 1 mm is considered normal (physiological anisocoria).
- In glaucoma patients who require regular monitoring of intraocular pressure (normal range 10 to 21 mmHg), RK correction is a relative contraindication because of the changed corneal biomechanical properties, which will cause underestimation.[21]
Equipment
Equipment needed for performing radial keratotomy are: topical anesthetic eye drops, gentian ink for corneal marking, optical zone marker, corneal incision marker, ultrasonic pachymeter, gem-quality diamond blade knife with 45-degree cutting angle, antibiotic and steroid eye drops.
Personnel
An interprofessional care team involved in the radial keratotomy procedure includes ophthalmic surgeons, optometrists, ophthalmic nurses/assistants, theatre staff, orthoptists, imaging technicians, and medical assistants.
Preparation
A thorough history and clinical examination are necessary to identify potential contraindications to surgery. It is also useful to take an occupational history and assess the patient's desires and expectations. Slit-lamp biomicroscopy will be undertaken of the ocular surface, including dry eye evaluation, intraocular pressure, cornea assessment, determination of cataract status, and dilated fundoscopic examination. During the preoperative workup, any contact lenses should be discontinued 1 to 2 weeks before corneal imaging to give more accurate measurements.[22] Corneal assessment with keratometry, topography, ultrasound pachymetry is standard practice.
Technique or Treatment
Pre-Surgery
Equipment needs to be checked for safety, and all patient data will need to be double-checked by clinical staff to minimize the risk of errors. Informed written consent is obtained from the patient, usually before the day of the procedure, so that there is adequate time to discuss any questions or concerns.
Surgical Technique
The basic elements of radial keratotomy are deceptively simple and comprise:
- Administration of appropriate anesthesia
- Accurate marking of the visual axis and incision lines taking into account any cyclotorsion, marking an appropriate size optical zone
- Measurement of the corneal thickness
- Accurate setting of the blade depth
- Making the corneal incisions,
- Administration of post-surgery antibiotic drops.
- Topical anesthesia is used for most patients, as this leaves the eye to remain mobile to mark the visual axis. The size of the optical zone is dependent on surgeon preference; in the PERK study, the clear central zone was determined by pre-operative spherical-equivalent cycloplegic refraction measuring 3 to 4 mm.[1] Corneal thickness is measured at 4 points paracentral at the determined optical zone in each quadrant, with an average of 3 readings taken to maximize accuracy. The diamond knife will be adjusted to the correct depth based on pachymetry measurements, and 8 incisions are usually made (less in smaller degrees of myopia). If there are post-operative under correction, additional incisions can then be considered. Radially placed incisions are used to correct myopia, with hexagonal incisions (hexagonal keratotomy) used for hyperopia.[23] Different methods of undertaking the incisions, from the initiating point, direction, depth, and length, have been proposed to improve results and long-term refractive stability.[24][25]
Post-Surgery
Post-operative eye drops were not routinely prescribed in the early years of radial keratotomy, which contributed to its popularity. Later topical steroids were used to accentuate the RK effect by modifying wound healing. If dry eye symptoms occur, they can be managed with topical ocular lubricants. The patient will be followed up with the surgeon, and studies have now confirmed that long-term refractive stability and vision quality is a challenge in post-RK patients.
Alternative Corneal Incisional Surgery
Astigmatic keratotomy (AK), also known as arcuate keratotomy, utilizes the placement of deep corneal incisions in the steep axis of astigmatism, resulting in flattening in the given meridian. A coupling effect occurs whereby steepening happens in the opposite and perpendicular meridian.[26] The relationship between the degree of flattening of the incised meridian to the steepening perpendicular meridian is known as the coupling ratio and is usually 1.[27] Incision depth is approximately 95% depth in the mid-peripheral cornea. AKs have been described in use after cataract surgery and post-penetrating keratoplasty in managing astigmatism.[28][29] Limbal relaxing incisions (LRIs) are set at 50 μm less than the thinnest measured pachymetry at the corneal limbus and have been described as a management option for astigmatism at the time of cataract surgery.[30] Modern developments involve the use of a femtosecond laser and nomograms to make these alternative incisions for improved accuracy.[31][32]
Complications
Sight-Threatening
These have been reported in 1% to 3% of eyes.[1] Bacterial and fungal keratitis, as well as endophthalmitis, have occurred after RK.[33][34][35] If full-thickness incisions were inadvertently made. This can lead to intraoperative trauma, cataract formation, and hemorrhage.[36] Decreased biomechanical stability at the points of incisions can lead to globe rupture through the keratotomy scars.[37] In the PERK study, 3% of eyes lost 2 or more lines of best-corrected visual acuity.[38]
Non-Sight-Threatening
Dry eyes can occur following radial keratotomy due to reduced tear production. This is caused by damage to the nerves from the incisions, which will affect the lacrimal reflex and the tear production cycle. Visual aberrations such as halo, glare, or light-bursts around lights, haze, and decreased contrast sensitivity can occur after radial keratotomy. Higher-order aberrations and increased pupil size are associated with radial keratotomy.[39] Long-term follow-up of radial keratotomy patients has revealed hyperopic regression at ten years post-surgery.[40] About 22% of eyes drifted 1.00 D or more towards hyperopia, and 2% of eyes drifted 1.00 D or towards myopia 6 months to 5 years after surgery in the PERK study.[38] Furthermore, diurnal variation has been reported in visual acuity, refraction, and topographic indexes 10 years post-RK.[41]
Clinical Significance
Patients who have had radial keratotomy correction are at risk of sight and non-sight threatening complications in the short and long term. The quality of vision can fluctuate during the day, and hyperopic regression occurs over time. The development of presbyopia and cataract will further exacerbate the challenges of visual rehabilitation for this group of patients. Methods for improving intraocular lens power calculations in post-RK patients have been described.[42] A modern iteration of radial keratotomy has been the use of asymmetric mini-RK as part of a treatment protocol for keratoconus.[43] Factors to consider include the underlying biomechanical stability of the cornea, which will affect measurements, presence of irregular astigmatism, size of the optic zone, and location of incisions. If there is significant corneal instability, irregularity, or scarring, initial collagen crosslinking treatment with or without therapeutic excimer laser ablation for scar removal may be necessary in order to facilitate accurate biometry measurements.
Enhancing Healthcare Team Outcomes
An interprofessional care team in radial keratotomy treatment consists of an ophthalmic surgeon, optometrist, nurses, and imaging technicians. The team identifies in outpatient clinics the appropriate candidates for the procedure and during the procedure itself adheres to clinical protocols. Patient education is the responsibility of the team with communication amongst team members being important throughout the process. [Level 5]
Nursing, Allied Health, and Interprofessional Team Interventions
The interprofessional team members will educate the patient about the radial keratotomy procedure followed by obtaining informed consent before proceeding to surgery. Instrumentation checks must be performed by the theatre staff, with asepsis guidelines followed. Communication and handover with other members of the team are essential to ensure safe standards of care.
Nursing, Allied Health, and Interprofessional Team Monitoring
Nursing and allied health staff will guide the patient through post-operative care by instructing the patient on the correct administration of eye drops. They will also explain to the patient red-flag symptoms to be aware of and of the need to contact the team should he/she develop them. They will be part of the patient follow-up in an outpatient setting, assisting with visual acuity assessments for safe monitoring.
Media
(Click Image to Enlarge)
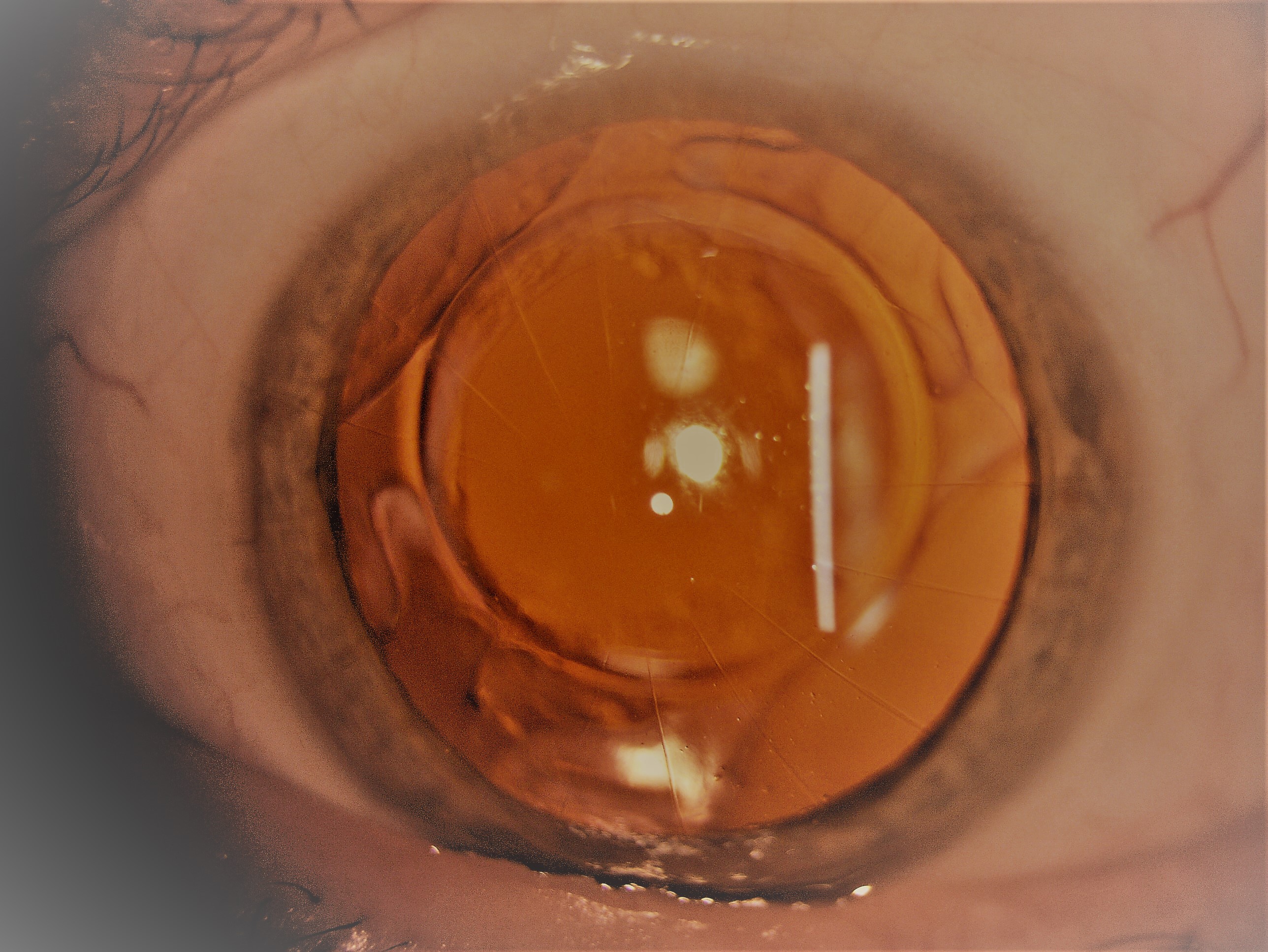
16-incision radial keratotomy in the left eye. The patient has had cataract surgery with implantation of an intraocular lens decades after the primary RK procedure. Contributed by Dr Lanxing Fu
(Click Image to Enlarge)
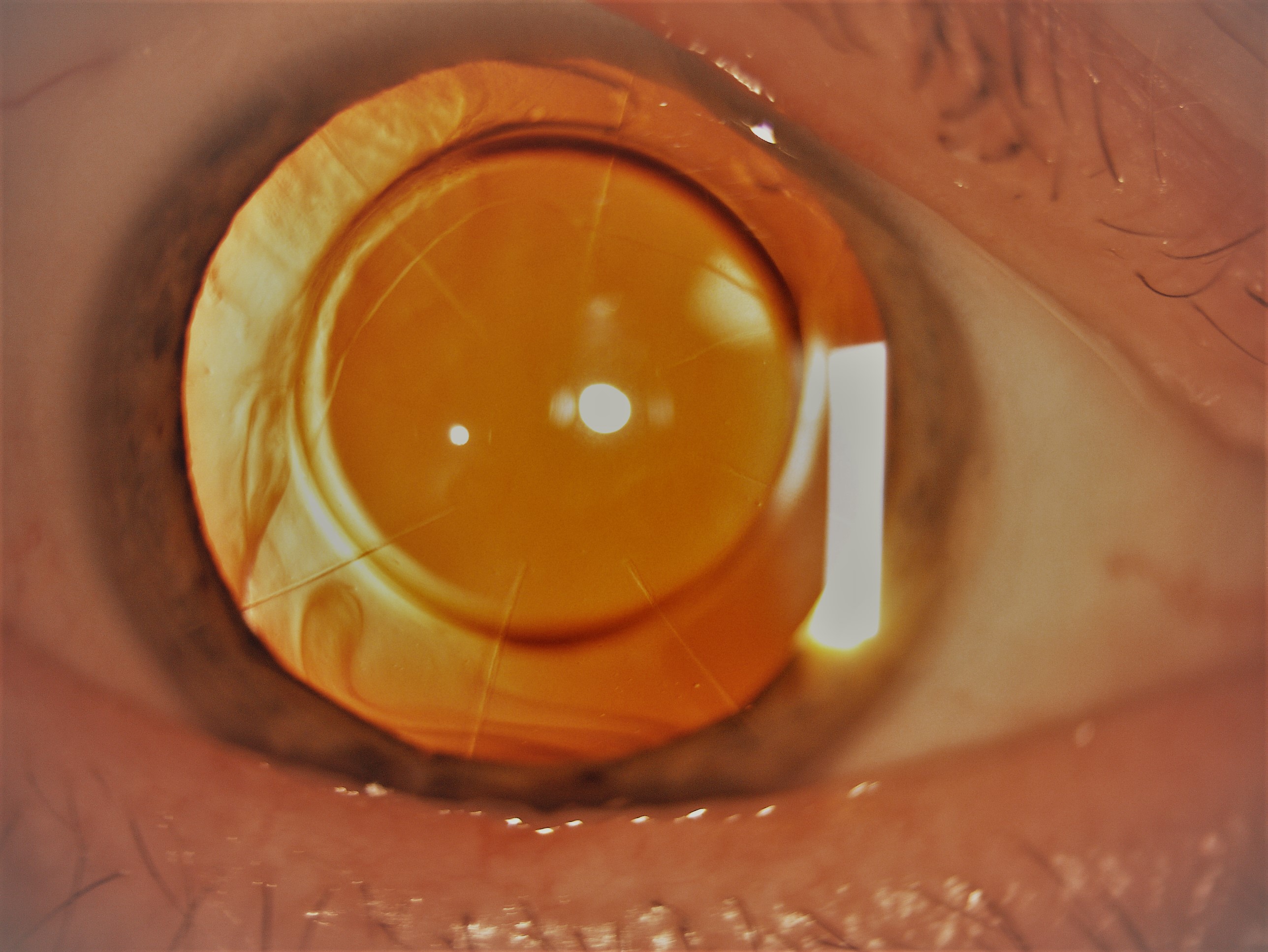
Standard 8-incision radial keratotomy with sparing of the pupillary zone. Contributed by Dr Lanxing Fu
References
Rowsey JJ, Morley WA. Surgical correction of moderate myopia: which method should you choose? I. Radial keratotomy will always have a place. Survey of ophthalmology. 1998 Sep-Oct:43(2):147-56 [PubMed PMID: 9763139]
Level 3 (low-level) evidenceSATO T. Posterior incision of cornea; surgical treatment for conical cornea and astigmatism. American journal of ophthalmology. 1950 Jun:33(6):943-8 [PubMed PMID: 15419252]
Beatty RF, Smith RE. 30-year follow-up of posterior radial keratotomy. American journal of ophthalmology. 1987 Mar 15:103(3 Pt 1):330-1 [PubMed PMID: 3826240]
Level 3 (low-level) evidenceFyodorov SN, Durnev VV. Operation of dosaged dissection of corneal circular ligament in cases of myopia of mild degree. Annals of ophthalmology. 1979 Dec:11(12):1885-90 [PubMed PMID: 556142]
Level 3 (low-level) evidenceBeliaev VS, Il'ina TS. [Scleroplasty in the treatment of progressive myopia]. Vestnik oftalmologii. 1972:3():60-3 [PubMed PMID: 5049984]
Enaliev FS. [Surgical treatment experience in myopia]. Vestnik oftalmologii. 1979 May-Jun:(3):52-5 [PubMed PMID: 462698]
Sawelson H, Marks RG. Two-year results of radial keratotomy. Archives of ophthalmology (Chicago, Ill. : 1960). 1985 Apr:103(4):505-10 [PubMed PMID: 3985827]
Bores LD, Myers W, Cowden J. Radial keratotomy: an analysis of the American experience. Annals of ophthalmology. 1981 Aug:13(8):941-8 [PubMed PMID: 7294635]
Bores LD. Radial keratotomy. I. A safe, effective way to correct a handicap. Survey of ophthalmology. 1983 Sep-Oct:28(2):101-5 [PubMed PMID: 6648792]
Level 3 (low-level) evidenceCowden JW. Radial keratotomy. A retrospective study of cases observed at the Kresge Eye Institute for six months. Archives of ophthalmology (Chicago, Ill. : 1960). 1982 Apr:100(4):578-80 [PubMed PMID: 7073568]
Level 2 (mid-level) evidenceWaring GO 3rd, Moffitt SD, Gelender H, Laibson PR, Lindstrom RL, Myers WD, Obstbaum SA, Rowsey JJ, Safir A, Schanzlin DJ, Bourque LB. Rationale for and design of the National Eye Institute Prospective Evaluation of Radial Keratotomy (PERK) Study. Ophthalmology. 1983 Jan:90(1):40-58 [PubMed PMID: 6338438]
Feizi S, Jafarinasab MR, Karimian F, Hasanpour H, Masudi A. Central and peripheral corneal thickness measurement in normal and keratoconic eyes using three corneal pachymeters. Journal of ophthalmic & vision research. 2014 Jul-Sep:9(3):296-304. doi: 10.4103/2008-322X.143356. Epub [PubMed PMID: 25667728]
Marfurt CF, Cox J, Deek S, Dvorscak L. Anatomy of the human corneal innervation. Experimental eye research. 2010 Apr:90(4):478-92. doi: 10.1016/j.exer.2009.12.010. Epub 2009 Dec 29 [PubMed PMID: 20036654]
Saghizadeh M, Kramerov AA, Svendsen CN, Ljubimov AV. Concise Review: Stem Cells for Corneal Wound Healing. Stem cells (Dayton, Ohio). 2017 Oct:35(10):2105-2114. doi: 10.1002/stem.2667. Epub 2017 Jul 26 [PubMed PMID: 28748596]
Khaled ML, Helwa I, Drewry M, Seremwe M, Estes A, Liu Y. Molecular and Histopathological Changes Associated with Keratoconus. BioMed research international. 2017:2017():7803029. doi: 10.1155/2017/7803029. Epub 2017 Jan 30 [PubMed PMID: 28251158]
Levy SG, Moss J, Sawada H, Dopping-Hepenstal PJ, McCartney AC. The composition of wide-spaced collagen in normal and diseased Descemet's membrane. Current eye research. 1996 Jan:15(1):45-52 [PubMed PMID: 8631203]
Tuft SJ, Coster DJ. The corneal endothelium. Eye (London, England). 1990:4 ( Pt 3)():389-424 [PubMed PMID: 2209904]
Level 3 (low-level) evidenceSalz JJ, Lee T, Jester JV, Villaseñor RA, Steel D, Bernstein J, Smith RE. Analysis of incision depth following experimental radial keratotomy. Ophthalmology. 1983 Jun:90(6):655-9 [PubMed PMID: 6888859]
Sutton G, Lawless M, Hodge C. Laser in situ keratomileusis in 2012: a review. Clinical & experimental optometry. 2014 Jan:97(1):18-29. doi: 10.1111/cxo.12075. Epub 2013 Jun 21 [PubMed PMID: 23786377]
Boxer Wachler BS, Durrie DS, Assil KK, Krueger RR. Improvement of visual function with glare testing after photorefractive keratectomy and radial keratotomy. American journal of ophthalmology. 1999 Nov:128(5):582-7 [PubMed PMID: 10577525]
Level 2 (mid-level) evidenceMaloley LA, Razeghinejad MR, Havens SJ, Gulati V, Fan S, High R, Ghate DA. Pneumotonometer Accuracy Using Manometric Measurements after Radial Keratotomy, Clear Corneal Incisions and Lamellar Dissection in Porcine Eyes. Current eye research. 2020 Jan:45(1):1-6. doi: 10.1080/02713683.2019.1652915. Epub 2019 Aug 22 [PubMed PMID: 31380714]
Wilkinson JM, Cozine EW, Kahn AR. Refractive Eye Surgery: Helping Patients Make Informed Decisions About LASIK. American family physician. 2017 May 15:95(10):637-644 [PubMed PMID: 28671403]
Grandon SC, Sanders DR, Anello RD, Jacobs D, Biscaro M. Clinical evaluation of hexagonal keratotomy for the treatment of primary hyperopia. Journal of cataract and refractive surgery. 1995 Mar:21(2):140-9 [PubMed PMID: 7791053]
Level 2 (mid-level) evidenceMelles GR, Binder PS. Effect of radial keratotomy incision direction on wound depth. Refractive & corneal surgery. 1990 Nov-Dec:6(6):394-403 [PubMed PMID: 2076416]
Level 3 (low-level) evidenceLindstrom RL. Minimally invasive radial keratotomy: mini-RK. Journal of cataract and refractive surgery. 1995 Jan:21(1):27-34 [PubMed PMID: 7722894]
Level 3 (low-level) evidenceThornton SP. Astigmatic keratotomy: a review of basic concepts with case reports. Journal of cataract and refractive surgery. 1990 Jul:16(4):430-5 [PubMed PMID: 2199665]
Level 3 (low-level) evidenceFaktorovich EG, Maloney RK, Price FW Jr. Effect of astigmatic keratotomy on spherical equivalent: results of the Astigmatism Reduction Clinical Trial. American journal of ophthalmology. 1999 Mar:127(3):260-9 [PubMed PMID: 10088734]
Level 2 (mid-level) evidenceOshika T, Shimazaki J, Yoshitomi F, Oki K, Sakabe I, Matsuda S, Shiwa T, Fukuyama M, Hara Y. Arcuate keratotomy to treat corneal astigmatism after cataract surgery: a prospective evaluation of predictability and effectiveness. Ophthalmology. 1998 Nov:105(11):2012-6 [PubMed PMID: 9818598]
Poole TR, Ficker LA. Astigmatic keratotomy for post-keratoplasty astigmatism. Journal of cataract and refractive surgery. 2006 Jul:32(7):1175-9 [PubMed PMID: 16857505]
Level 2 (mid-level) evidenceBudak K, Yilmaz G, Aslan BS, Duman S. Limbal relaxing incisions in congenital astigmatism: 6 month follow-up. Journal of cataract and refractive surgery. 2001 May:27(5):715-9 [PubMed PMID: 11377902]
Kumar NL, Kaiserman I, Shehadeh-Mashor R, Sansanayudh W, Ritenour R, Rootman DS. IntraLase-enabled astigmatic keratotomy for post-keratoplasty astigmatism: on-axis vector analysis. Ophthalmology. 2010 Jun:117(6):1228-1235.e1. doi: 10.1016/j.ophtha.2009.10.041. Epub 2010 Feb 16 [PubMed PMID: 20163860]
Level 2 (mid-level) evidenceLim CW, Somani S, Chiu HH, Maini R, Tam ES. Astigmatic Outcomes of Single, Non-Paired Intrastromal Limbal Relaxing Incisions During Femtosecond Laser-Assisted Cataract Surgery Based on a Custom Nomogram. Clinical ophthalmology (Auckland, N.Z.). 2020:14():1059-1070. doi: 10.2147/OPTH.S238016. Epub 2020 Apr 22 [PubMed PMID: 32368004]
Beldavs RA, al-Ghamdi S, Wilson LA, Waring GO 3rd. Bilateral microbial keratitis after radial keratotomy. Archives of ophthalmology (Chicago, Ill. : 1960). 1993 Apr:111(4):440 [PubMed PMID: 8470970]
Level 3 (low-level) evidenceMaskin SL, Alfonso E. Fungal keratitis after radial keratotomy. American journal of ophthalmology. 1992 Sep 15:114(3):369-70 [PubMed PMID: 1524133]
Level 3 (low-level) evidenceGelender H, Flynn HW Jr, Mandelbaum SH. Bacterial endophthalmitis resulting from radial keratotomy. American journal of ophthalmology. 1982 Mar:93(3):323-6 [PubMed PMID: 6978616]
Level 3 (low-level) evidenceRashid ER, Waring GO 3rd. Complications of radial and transverse keratotomy. Survey of ophthalmology. 1989 Sep-Oct:34(2):73-106 [PubMed PMID: 2686058]
Level 3 (low-level) evidenceMcDermott ML, Wilkinson WS, Tukel DB, Madion MP, Cowden JW, Puklin JE. Corneoscleral rupture ten years after radial keratotomy. American journal of ophthalmology. 1990 Nov 15:110(5):575-7 [PubMed PMID: 2240150]
Level 3 (low-level) evidenceWaring GO 3rd, Lynn MJ, Nizam A, Kutner MH, Cowden JW, Culbertson W, Laibson PR, McDonald MB, Nelson JD, Obstbaum SA. Results of the Prospective Evaluation of Radial Keratotomy (PERK) Study five years after surgery. The Perk Study Group. Ophthalmology. 1991 Aug:98(8):1164-76 [PubMed PMID: 1923352]
Applegate RA, Howland HC, Sharp RP, Cottingham AJ, Yee RW. Corneal aberrations and visual performance after radial keratotomy. Journal of refractive surgery (Thorofare, N.J. : 1995). 1998 Jul-Aug:14(4):397-407 [PubMed PMID: 9699163]
Waring GO 3rd, Lynn MJ, McDonnell PJ. Results of the prospective evaluation of radial keratotomy (PERK) study 10 years after surgery. Archives of ophthalmology (Chicago, Ill. : 1960). 1994 Oct:112(10):1298-308 [PubMed PMID: 7945032]
Level 1 (high-level) evidenceKemp JR, Martinez CE, Klyce SD, Coorpender SJ, McDonald MB, Lucci L, Lynn MJ, Waring GO 3rd. Diurnal fluctuations in corneal topography 10 years after radial keratotomy in the Prospective Evaluation of Radial Keratotomy Study. Journal of cataract and refractive surgery. 1999 Jul:25(7):904-10 [PubMed PMID: 10404364]
Turnbull AMJ, Crawford GJ, Barrett GD. Methods for Intraocular Lens Power Calculation in Cataract Surgery after Radial Keratotomy. Ophthalmology. 2020 Jan:127(1):45-51. doi: 10.1016/j.ophtha.2019.08.019. Epub 2019 Aug 23 [PubMed PMID: 31561878]
Abbondanza M, Abbondanza G, De Felice V, Wong ZSY. Long-term Results of Mini Asymmetric Radial Keratotomy and Corneal Cross-linking for the Treatment of Keratoconus. Korean journal of ophthalmology : KJO. 2019 Apr:33(2):189-195. doi: 10.3341/kjo.2018.0028. Epub [PubMed PMID: 30977329]