 Ultrasound-Guided Fascia Iliaca Compartment Block
Ultrasound-Guided Fascia Iliaca Compartment Block
Introduction
Pain management is an integral part of providing care in the emergency setting. Lower extremity pain from hip fractures, burns, and other trauma is a common presenting complaint. Unfortunately, pain management can be difficult due to medication side effects, patient preferences, and other patient characteristics that can make intravenous analgesia less desirable. Opioid medications can be associated with respiratory depression, hypotension, mental status changes, and vomiting. NSAIDs can increase bleeding risk and exacerbate underlying gastrointestinal (GI) problems. Acetaminophen alone is often not sufficient for severe pain. Hip fractures, in particular, can cause considerable pain, and often occur in elderly adults with multiple comorbidities which make analgesia challenging.
A fascia iliaca compartment block can provide superior analgesia with minimal side effects. It can be deployed in a relatively quick fashion after a small amount of training and can be executed with high success rates under ultrasound guidance. In a study by Monzon et al., patients who received a fascia iliaca compartment block for a hip fracture had significantly reduced pain levels.[1] The pain was initially rated at an average of 8.5 on a 10 point scale but decreased to an average of 2.3 at 2 hours post-injection. In a study by Stevens et al., in Anesthesia Intensive Care, patients who underwent a fascia iliaca compartment block used significantly less morphine over the course of 24 hours than the control group which used morphine alone.[2] An additional advantage is the duration of effect, which has been seen for 8 to 10 hours following a single shot block. Another randomized placebo-controlled trial showed that pain relief was superior at all time points measured in the fascia iliac compartment block group as compared with a group utilizing morphine only. In fact, median total morphine consumption in the compartment block group was 0 mg due to excellent analgesia after only a compartment block. Similar results were seen in a study by Lopez et al. for femoral shaft fractures. Emergency department-specific studies using ultrasound guidance have shown 76% mean reduction of pain score in patients with hip fracture at 120 minutes.[3][4]
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
Sensory innervation to the lower extremity is handled through the sciatic nerve, femoral nerve, obturator nerve, and lateral femoral cutaneous nerve. These originate from the lumbar plexus, except for the sciatic nerve, which receives some contribution from the sacral plexus.
The femoral nerve is the largest of the four nerves and is commonly identified on ultrasound by emergency physicians when placing central venous access into the femoral vein. It is situated just lateral to the femoral artery on top of the iliac is muscle. The fascia iliaca separates the femoral nerve from the femoral artery.
- The obturator nerve runs through the psoas muscle and wraps behind the common iliac vessels. It affects only a minute portion of the medial aspect of the leg. The obturator nerve is variably blocked when performing the fascia iliaca compartment block.
- The lateral femoral cutaneous nerve innervates the lateral aspect of the thigh. This nerve runs behind the lateral aspect of the inguinal ligament.
- The sciatic nerve innervates the posterior compartment of the thigh. Because of its location, it is not blocked by anesthetic injection anteriorly.
The fascia iliaca is the second fascial plane encountered when viewing the proximal lower extremity under ultrasound. It runs below the fascia lata. In blind approaches, a characteristic "2 pops" are felt which indicates entrance into the compartment. The fascia iliaca runs anterior to the iliac this muscle, psoas muscle, and pectineus muscle. The sartorius muscle, as well as the femoral vessels, is located between the fascia lata and the fascia iliac. The fascia iliac compartment block has the potential to create a sensory block of the femoral, obturator, genitofemoral, and lateral femoral cutaneous nerves.
Indications
This compartment block can be considered with any painful trauma or procedures in the lower extremity within the nervous distribution noted above. It is especially helpful in cases where opioid analgesics are not ideal or contraindicated. It can also be used in conjunction with opioids for difficult to control pain. Specific indications which have been studied include hip fractures, femoral shaft fractures, and burns.
Contraindications
- Patient unwillingness to consent to the procedure
- Known allergy to local anesthetics
- Local anesthetic injection which has already approached the maximum dosage
- Previous femoral bypass surgery
- Local infection at the injection site
- Anticoagulation (relative)
Equipment
- Portable ultrasound machine with a linear high-frequency transducer
- Surgical marking pen
- Sterile probe covers
- Chlorhexidine solution, Betadine, or other antiseptic solution
- Spinal needle or nerve block specific needle
- 30-gauge short needle
- Three mL syringe
- 20 to 60 mL syringe
- Long-acting local anesthetic
- Cardiac monitor with continuous pulse oximetry
- Intralipid and plan for local anesthetic toxicity response
Personnel
Past literature has supported the effectiveness of regional anesthesia by both anesthesiologists as well as emergency physicians. More recent studies have shown that resident physicians can reliably perform a fascia iliaca compartment block after minimal amounts of training. A study published in the Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine has shown that prehospital EMS nurses can also demonstrate competency in a fascia iliaca compartment blocks using a blind technique.
Preparation
Preparation is necessary for achieving a successful and safe compartment block. As with any other procedure, the risks and benefits of the proposed procedure should be explained to the patient in terms they can easily understand. Time should be taken to answer any questions they may have. Written consent should be obtained at that time. If deemed appropriate, a small dose of an anxiolytic may assist in relieving any pre-procedure anxiety and facilitate proper positioning and cooperation. A detailed neurovascular exam of the lower extremity should be obtained before the start of the procedure. The site of the planned compartment block should be marked with a surgical marking pen and initialed by the provider intending to complete the procedure. The equipment and supplies necessary for completing the procedure should be collected and set up in the room (see above).
Technique or Treatment
The authors have utilized the following techniques and found them to be effective. The authors recognize that there are many successful strategies which have been employed to perform this block and alternative techniques may be equally appropriate.
- Explain the procedure and obtaining written consent as noted above.
- Document detailed neurovascular exam.
- Ensure all needed supplies are at the bedside.
- Perform timeout procedure with additional clinician or nurse.
- Administer a small dose of intravenous anxiolytic if appropriate and deemed necessary.
- Identify the neurovascular bundle utilizing ultrasound with the probe marker to the patient's right and mark the femoral artery with the surgical marking pen.
- Place sterile gloves, and with the help of an assistant, apply a sterile probe cover to the ultrasound.
- Clean the area using an antiseptic solution in the usual sterile fashion and place small sterile drapes.
- Again, identify the femoral vessels with ultrasound and then slide the probe laterally, away from the neurovascular bundle. This is done while at all times, keeping the fascia iliaca in view.
- Place a small amount of 1% lidocaine using the 30-gauge short needle to form a skin wheal in the intended area of injection.
- Fill a large syringe connected to a spinal needle or nerve block needle with long-acting local anesthetic. Be sure not to exceed maximum dosing of local anesthetic. The authors have found that 20 mL of 0.5% bupivacaine mixed with 10 mL of sodium chloride solution is generally safe and effective for an average sized adult.
- Insert the needle in the area of the previously created skin wheal in an in-plane technique. The needle tip should be in constant view under dynamic ultrasound guidance. Advance the needle until the fascia iliaca has just been punctured.
- Withdraw/aspirate to ensure that there is no blood return indicating entrance into a vessel.
- Carefully inject a small amount of anesthetic and observe the separation of the fascia iliaca from the underlying muscle planes. Continue to inject and aspirate every 5 mL to ensure correct placement. The anesthetic should flow easily into the space with a minimal amount of resistance. There should never be any blood return when checking aspiration. The provider may periodically elect to move the transducer more medially to view the anesthetic surrounding the femoral nerve directly. If this is done, the injection should pause, and the needle should be held in place without any advancement or retraction until the ultrasound is moved back to view the needle tip.
- During the procedure, the clinician should frequently evaluate the cardiac monitor for any signs of ectopy. If any ectopy is noted, the injection should immediately cease. Additionally, the clinician may want to ask the patient about any symptoms of local anesthetic toxicity such as lightheadedness, dizziness, perioral numbness or tingling. This assessment should repeat at the end of the procedure. If any signs of local anesthetic toxicity are observed, help should be requested and Intralipid should be considered.
- Following the procedure, a repeat neurovascular exam should be documented in the procedure note completed. The clinician should note the time of the block in their procedure note, as well as marking it with a surgical marking pen at the site of injection.
Complications
Overall complication rates are low. In an emergency department study of 63 adult patients who underwent single fascia iliac compartment block by resident physicians after 5 minutes of instruction, there were no systemic complications found and only two local hematomas.[5] Even when the procedure was performed blindly by EMS nurses in the prehospital setting, there were no complications noted in a study enrolling 100 patients.[6] The distance at which the skin is punctured from the neurovascular bundle minimizes the risk of intravascular injection or nerve transection. Intravascular injection or nerve damage is exceedingly rare.
Clinical Significance
The fascia iliaca compartment block is ideally suited for the emergency department setting in that it can be utilized quickly and effectively. It has the potential to provide lasting pain relief with minimal side effects. Ultrasound guidance can improve the accuracy of anesthetic injection and increase procedural safety. The skills of ultrasound guidance for needle placement are already utilized by emergency physicians and can easily be applied to this important but often underutilized setting.
Enhancing Healthcare Team Outcomes
Fascia lata compartment blocks are often performed by an anesthesiologist, emergency department physicians, neurologists, orthopedic surgeons, and pain specialist. However, anyone who performs this block must have a dedicated nurse for monitoring the patient throughout the procedure. While complications are rare, resuscitative equipment must be in the room before starting the procedure. The fascia lata block is effective and produces reliable analgesia.[7][8][9][10] (Level V)
Media
(Click Image to Enlarge)
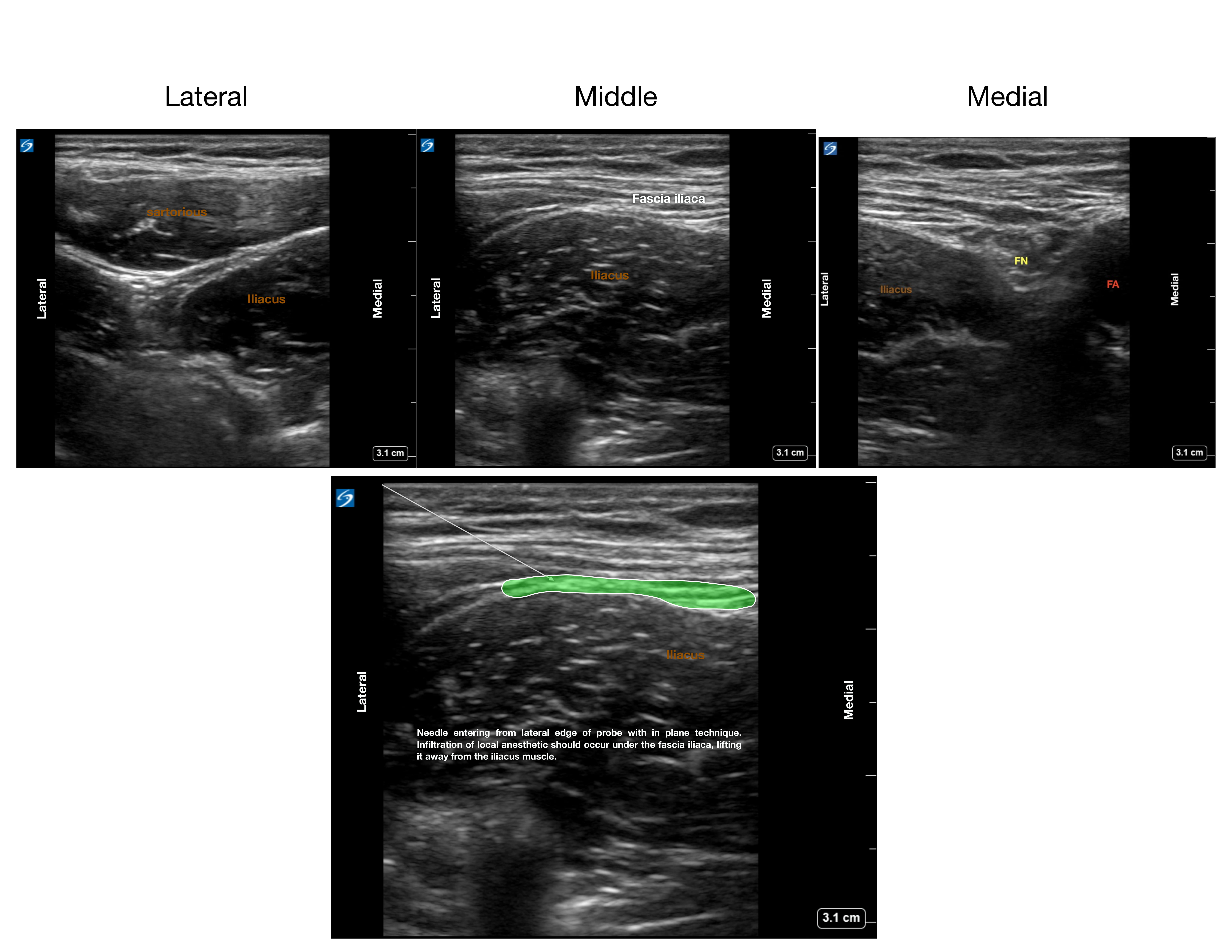
Anatomy of the fascia iliaca and ideal needle positioning Contributed by Neil Madhani, MD
References
Godoy Monzon D, Iserson KV, Vazquez JA. Single fascia iliaca compartment block for post-hip fracture pain relief. The Journal of emergency medicine. 2007 Apr:32(3):257-62 [PubMed PMID: 17394987]
Stevens M, Harrison G, McGrail M. A modified fascia iliaca compartment block has significant morphine-sparing effect after total hip arthroplasty. Anaesthesia and intensive care. 2007 Dec:35(6):949-52 [PubMed PMID: 18084988]
Level 1 (high-level) evidenceFoss NB, Kristensen BB, Bundgaard M, Bak M, Heiring C, Virkelyst C, Hougaard S, Kehlet H. Fascia iliaca compartment blockade for acute pain control in hip fracture patients: a randomized, placebo-controlled trial. Anesthesiology. 2007 Apr:106(4):773-8 [PubMed PMID: 17413915]
Level 1 (high-level) evidenceHaines L, Dickman E, Ayvazyan S, Pearl M, Wu S, Rosenblum D, Likourezos A. Ultrasound-guided fascia iliaca compartment block for hip fractures in the emergency department. The Journal of emergency medicine. 2012 Oct:43(4):692-7. doi: 10.1016/j.jemermed.2012.01.050. Epub 2012 Apr 9 [PubMed PMID: 22494596]
Høgh A, Dremstrup L, Jensen SS, Lindholt J. Fascia iliaca compartment block performed by junior registrars as a supplement to pre-operative analgesia for patients with hip fracture. Strategies in trauma and limb reconstruction. 2008 Sep:3(2):65-70. doi: 10.1007/s11751-008-0037-9. Epub 2008 Sep 2 [PubMed PMID: 18762870]
Dochez E, van Geffen GJ, Bruhn J, Hoogerwerf N, van de Pas H, Scheffer G. Prehospital administered fascia iliaca compartment block by emergency medical service nurses, a feasibility study. Scandinavian journal of trauma, resuscitation and emergency medicine. 2014 Jun 23:22():38. doi: 10.1186/1757-7241-22-38. Epub 2014 Jun 23 [PubMed PMID: 24957807]
Level 2 (mid-level) evidenceAluisio AR, Teicher C, Wiskel T, Guy A, Levine A. Focused Training for Humanitarian Responders in Regional Anesthesia Techniques for a Planned Randomized Controlled Trial in a Disaster Setting. PLoS currents. 2016 Nov 16:8():. pii: ecurrents.dis.e75f9f9d977ac8adededb381e3948a04. doi: 10.1371/currents.dis.e75f9f9d977ac8adededb381e3948a04. Epub 2016 Nov 16 [PubMed PMID: 28018749]
Level 1 (high-level) evidenceGasanova I, Alexander JC, Estrera K, Wells J, Sunna M, Minhajuddin A, Joshi GP. Ultrasound-guided suprainguinal fascia iliaca compartment block versus periarticular infiltration for pain management after total hip arthroplasty: a randomized controlled trial. Regional anesthesia and pain medicine. 2019 Feb:44(2):206-211. doi: 10.1136/rapm-2018-000016. Epub [PubMed PMID: 30700615]
Level 1 (high-level) evidenceSivakumar RK, Panneerselvam S, Cherian A, Rudingwa P, Menon J. Perineural vs. intravenous dexmedetomidine as an adjunct to bupivacaine in ultrasound guided fascia iliaca compartment block for femur surgeries: A randomised control trial. Indian journal of anaesthesia. 2018 Nov:62(11):851-857. doi: 10.4103/ija.IJA_397_18. Epub [PubMed PMID: 30532320]
Level 1 (high-level) evidenceMa YH, Wu J, Jia B, Xue JX, Wang TL. [Continuous fascia iliaca compartment block combined with oral analgesics for pre-operative pain control in elderly hip fracture patients]. Zhonghua yi xue za zhi. 2018 Mar 13:98(10):723-727. doi: 10.3760/cma.j.issn.0376-2491.2018.10.002. Epub [PubMed PMID: 29562394]