 Anatomy, Bony Pelvis and Lower Limb: Leg Bones
Anatomy, Bony Pelvis and Lower Limb: Leg Bones
Introduction
The leg is the region of the lower limb between the knee and the foot. It comprises two bones: the tibia and the fibula. The role of these two bones is to provide stability and support to the rest of the body, and through articulations with the femur and foot/ankle and the muscles attached to these bones, provide mobility and the ability to ambulate in an upright position. The tibia articulates with the femur at the knee joint. The knee joint consists of three compartments.[1][2]
- Medial tibiofemoral compartment
- Lateral tibiofemoral compartment
- Patellofemoral compartment
At the ankle, the tibia and fibula create the articular surface for the talus. The ankle mortise is a specialized articulation providing support and optimizing motion and function through the ankle joint. A normal ankle joint ultimately optimizes and allows for physiologic mobility of the foot and its associated joints and articulations. The bones and fascia also divide the lower leg into four compartments [3][4]
- Anterior compartment
- Lateral compartment
- Posterior compartment, superficial
- Posterior compartment, deep
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The tibia is the second largest bone in the body and provides support for a significant portion of the weight-bearing forces transmitted from the rest of the body. Proximally in cross-section, the tibia assumes a pyramidal shape/surface that articulates with the femur at the knee joint. The proximal tibia consists of medial and lateral tibial plateau surfaces, each with an associated meniscus. In the center of the two plateaus is an intercondylar spine, which contains a portion of the attachment footprint for the anterior cruciate ligament (ACL). The posterior portion contains a corresponding portion for the attachment footprint of the posterior cruciate ligament (PCL).[2] These ligaments attach the femur to the tibia.
In addition to the ACL and PCL, knee joint stability in the coronal plane is a function of the medial collateral ligament (MCL) and the lateral collateral ligament (LCL). The MCL spans from the medial aspect of the femur to the proximal tibia distal to the joint line. The LCL attaches to the lateral aspect of the femur and courses to the anterolateral fibula head.[5] The patellar tendon also attaches to the proximal tibia.[6] This tendon inserts on the tibial tubercle at the midline on the tibia directly distal to the knee joint. The posterior aspect of the knee provides, in general, stability for the knee in extension. Posterior support of the knee joint is critical as the popliteal region includes the neurovascular bundle, which passes through this area to provide significant neurovascular contributions to the lower leg and foot.[7][8]
The fibula is much smaller and provides much less weight-bearing support compared to its tibial counterpart. The fibula connects to the tibia via an interosseous membrane that connects the two bones distally at the ankle joint. Proximally, the proximal tibiofibular joint serves as the proximal anchoring stabilizing connection between the two bones in the lower leg.
The fibula forms the lateral border of the ankle joint while the tibia forms the medial border. Relative to the ankle joint, these osseous segments are referred to as the lateral and medial malleoli, respectively.[9] The osseous integrity of the malleoli and the ankle syndesmosis (including the interosseous membrane and syndesmotic ligaments) serve to provide a seamless and confluent ankle mortise that optimizes the delicate balance of tibiotalar mobility and stability. The medial malleolus provides attachment points for the large deltoid ligament, the posterior tibiotalar ligament, the tibiocalcaneal ligament, and the tibionavicular ligament. The lateral malleolus provides an attachment for the anterior talofibular ligament, the calcaneofibular ligament, and the posterior talofibular ligament.
Embryology
The lower limbs form in the fourth week of prenatal development. They develop in a cranial to caudal direction. Ossification centers form in the tibia around the sixth week, and during the seventh or eighth week in the fibula. Each bone forms via endochondral ossification. The fusion of the ossification centers starts around the sixteenth year of life, with the proximal ossification center fusing before the distal ossification centers. The fusion of the ossification centers completes normal bone growth.
Blood Supply and Lymphatics
The popliteal artery is the continuation of the superficial femoral artery and is the blood supply below the knee. It begins in the popliteal fossa, inferior to the popliteus muscle. The branches of the popliteal artery are the anterior tibial artery, posterior tibial artery, sural arteries, medial superior genicular artery, lateral superior genicular artery, middle genicular artery, lateral inferior genicular artery, and medial inferior genicular artery. The arterial supply to the tibia is multifaceted. Branches of the anterior tibial artery supply the proximal metaphysis and epiphysis from the periphery via periosteal branches. The nutrient artery supplies the diaphysis. This artery penetrates the tibia posteriorly, distal to the soleal line near the center of the tibia, and sends branches towards the proximal and distal ends of the diaphysis [3]. The penetrating branches of the posterior tibial artery supply the distal metaphysis and epiphysis from the periphery.[10]
The arterial supply of the proximal epiphysis and metaphysis of the fibula is through branches of the anterior tibial artery and more distally by the fibular artery. This blood supply is noteworthy as graft reconstruction surgery of the mandible often uses the proximal fibula.
Venous drainage of the tibia is via the anterior and posterior tibial veins, and fibula drainage is via the fibular vein. These veins drain into the popliteal vein.
The lymphatic drainage of the tibia and fibula is to the superficial and deep inguinal lymph nodes.
Nerves
Branches from the tibial nerve that supply the knee joint provide innervation to the proximal tibia. Distally, branches from nerves supplying the overlying muscle innervate the tibia below. These are branches of the deep femoral nerve and the tibial nerve. The sciatic nerve divides just proximal to the popliteal fossa into the common peroneal (fibular) and tibial nerve—the common peroneal nerve winds around the fibular neck. The peroneal nerve innervates the posterior lateral lower leg. It allows for eversion and dorsiflexion. The superficial peroneal nerve is a cutaneous branch of the peroneal nerve and is responsible for sensation to the upper two-thirds of the posterior lateral leg.[11]
Branches of the superficial peroneal nerve terminate at the deep crural fascia, dividing into the medial and intermediate dorsal cutaneous nerves. These nerves supply the dorsal surface on the foot, with exception to the dorsal webbed space between the first and second toe.[12] The deep peroneal nerve innervates the first and second toe webbed space. The tibial nerve is responsible for inversion and plantar flexion. The sural nerve is a cutaneous branch of the tibial nerve and provides sensory for the anteromedial lower leg. Cutaneous branches of the tibial nerve provide sensation to most of the plantar surface of the foot.[13]
Muscles
Muscles demonstrating origin/insertion footprints on the tibia include [14][15][16][17][18][19]
- Tensor fasciae latae inserts on the lateral (Gerdy) tubercle of the tibia.
- Quadriceps femoris inserts anteriorly on the tibial tuberosity.
- Sartorius, gracilis, and semitendinosus insert anteromedially on the pes anserinus.
- Horizontal head of semimembranosus muscle inserts on the medial condyle.
- Popliteus inserts on the soleal line of the posterior tibia.
- Tibialis anterior originates at the upper two-thirds of the lateral tibia.
- Extensor digitorum longus originates at the lateral condyle of the tibia.
- Soleus and flexor digitorum longus originate at the posterior aspect of the tibia on the soleal line.
Muscles associated with the fibula:
- The biceps femoris tendon inserts on the fibular head.
- The fibularis longus and fibularis brevis tendons insert on the lateral fibula.
- The extensor digitorum longus and extensor hallucis longus tendons insert on the medial fibula.
- The fibularis tertius (FT) is a small muscle in the anterior compartment of the leg that inserts on the anterior surface of the distal fibula.[20]
Surgical Considerations
Tibial Fractures
Fractures involving the tibia are relatively common injuries. Tibial plateau fractures are proximal tibial fractures with extension into the articular surface. In general, these fractures have significant associated morbidity and long-term implications that can significantly impact patient function and outcomes. For example, tibial plateau fractures correlate with [21]
- Meniscal tears:
- Lateral meniscal tears
- More commonly associated lateral tibial fractures (e.g., Schatzker II pattern)
- Associated with greater than 10mm of articular depression
- medial meniscal tears
- More commonly associated with medial tibial plateau fractures (e.g., Schatzker IV pattern)
- ACL injuries
- Compartment syndrome
- Vascular injury
- Lateral meniscal tears
Operative fixation is often necessary for the setting of increasing displacement and associated injury. [22] Post-traumatic deformity and/or end-stage arthritis is not tolerated without subsequent orthopedic intervention in these patients. End-stage arthritic changes and deformity require a spectrum of reconstructive knee options, such as total knee arthroplasty (TKA).[1] In the appropriate patient, TKA is a consistently successful and reproducible procedure that can restore mobility and function these debilitated patients.[23][24]
Tibial shaft fractures can occur and are often open due to the proximity to the skin of the tibia. Operative treatment may be required, consisting of open reduction internal fixation (ORIF) with plate/screws, external fixation, or intramedullary nail fixation.[25]
Ankle Fractures
Ankle fractures, in general, constitute a wide range of injury patterns, bony/ligamentous involvement, and potential instability.[9] Mechanisms of injury often include some combination of rotational force(s) combined with inversion or eversion pathologic positioning at the time of injury and fracture. Although the comprehensive treatment/workup is beyond the scope of this review, ankle fractures are diagnosed utilizing a combination of patient-reported history, the presence of deformity/pain on the exam, and radiographic imaging. A 2017 systematic review with meta-analysis investigating the diagnostic accuracy of the Ottawa Ankle Rules demonstrated that the sensitivity of the scoring system was more sensitive in adults compared to children, and the influence of subspecialty profession by the healthcare provider had a negligible influence on the overall diagnostic accuracy. The authors concluded that, across the 66 included studies in the review, the ankle rules consistently demonstrated high sensitivity and a low negative likelihood ratio, indicating that a negative test result is highly informative in excluding a fracture of the ankle, thus preventing the need for further radiographic imaging.[26]
Fibular Grafting
The advantage of the fibula being a large, relatively non-weight-bearing bone is clear in its use as a bone graft during mandibular reconstruction; this is the “gold standard” with several variations in the surgery in development. The fibula has a large amount of dense cortical bone that is easily accessible and a highly vascularized intrinsic blood supply that will decrease union time. This vascularity has shown superiority to non-vascular bone grafts in both functionality and aesthetics.[27]
Fibular strut grafts are also often utilized in various procedures to augment surgical fixation in the setting of comminuted fragility fractures (i.e., those occurring secondary to osteoporosis or low bone mineral density.)[28][29] For example, fibular strut grafting is a common choice in osteopenic patients with comminuted proximal humerus fractures undergoing ORIF with plate/screws.[30][28]
Clinical Significance
Medial tibial stress syndrome is the most commonly known case of tibial periostitis and is better known as shin splints. Shin splints are periostitis of the tibia from repetitive use. A chief complaint of new physical activity like running, after prolonged periods of inactivity, is the usual cause. The pathology is also present in dancers, or any activity requiring an overload of the lower extremities. The posteromedial surface of the tibia is the most common location of the inflammation. Patients will often describe the pain as sharp, non-radiating, and is elicited by their inducing activity. The pain will normally last the length of the activity, and shortly after, the patient chooses to rest.
Physical and anatomical variances like obesity and hyperpronated (flat) arches put an individual at risk. Also, improper footwear and gait abnormalities increase the propensity to develop shin splints. The physical exam is important to separate shin splints from other pathologies like fractures. Palpating the length of the tibia, anteromedially and posteromedially, is important. Pain and tenderness are present on the exam. In severe cases, nodules can be palpable. Sometimes, manipulation of the ankle and assessing for tightness in soleus and gastrocnemius can be an indication for shin splints. Rest, ice, compression, and nonsteroidal anti-inflammatory drugs (NSAIDs) are the mainstay of shin splint management, in that order. Shin splints pain that is resistant to conservative management or pain that occurs outside of inducing activity may require imaging to rule out a stress fracture and other pathologies.[25]
Tibial stress fractures have a similar presentation to shin splints. The epidemiology is also similar, with the addition of avid runners, and people with low BMIs. An X-ray is the first-line, but inconclusive imaging modality. X-rays often miss stress fractures, especially in the initial inflammatory period. The patient can undergo another X-ray after 2 to 3 weeks, or if an urgent diagnosis is needed, they can opt for an MRI. An MRI is the most sensitive imaging modality for tibial stress fractures and can aid in excluding other pathologies like acute compartment syndrome.[25] [31] Bone scintigram scan can also be performed to highlight a stress fracture. The conservative management for stress fractures is the same as shin splints. However, patients are to refrain from running or stressful activities to the leg for 6 to 8 weeks. Patients may also wear a pneumatic brace when they return to activity.[32]
Apophysitis of the tibial tubercle, or Osgood-Schlatter disease, is another pain syndrome of the tibia. The pain is located directly below the knee with that, like shin splints, gets worse with activity and improves with rest; this is the point where the patellar tendon inserts on the tibia and can become stressed with repeated use of the knee. A palpable bony prominence can be present, and palpation to this point can be extremely painful. Rest and ice are the mainstays of treatment. Since this syndrome is most common in ten to fifteen-year-olds, the symptoms usually resolve as the epiphyseal plates close.[25][6]
Compartment syndrome is a significant complication of tibial fractures and other traumas to the leg. Following the trauma, blood and other fluids fill the compartments created by the thick fascia and bones. This increased fluid within the compartments causes an increase in pressure that can compress the venous return, which can lead to tissue ischemia and cellular death.[33] Within six to eight hours of compression, irreversible damage to the muscles and nerves within the compartments. Monitoring the intramuscular pressure is the current basis of diagnosis, although other methods are under investigation. The mainstay of treatment is rapid fasciotomy to decrease pressure and restore venous return.[34]
Media
(Click Image to Enlarge)
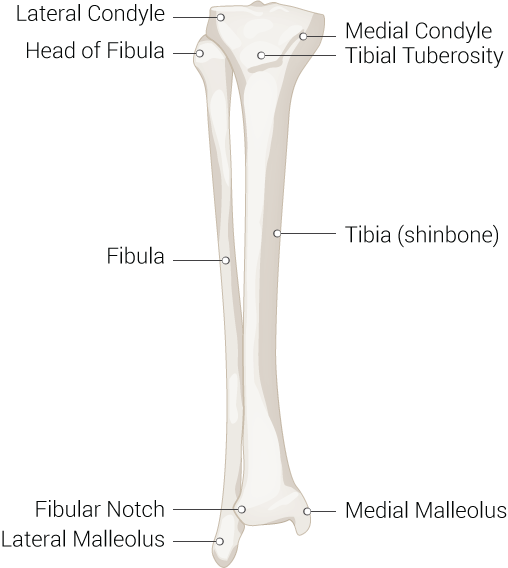
Inferior Leg Bones. Leg bone anatomy including the tibia, fibula, fibular notch, lateral malleolus, medial malleolus, lateral condyle, medial condyle, tibial tuberosity, and head of fibula.
Contributed by Beckie Palmer
References
Varacallo M, Luo TD, Johanson NA. Total Knee Arthroplasty Techniques. StatPearls. 2023 Jan:(): [PubMed PMID: 29763071]
Raj MA, Mabrouk A, Varacallo M. Posterior Cruciate Ligament Knee Injuries. StatPearls. 2023 Jan:(): [PubMed PMID: 28613477]
Binstead JT, Munjal A, Varacallo M. Anatomy, Bony Pelvis and Lower Limb: Calf. StatPearls. 2023 Jan:(): [PubMed PMID: 29083629]
Bordoni B, Varacallo M. Anatomy, Bony Pelvis and Lower Limb, Gastrocnemius Muscle. StatPearls. 2023 Jan:(): [PubMed PMID: 30422541]
Hyland S, Varacallo M. Anatomy, Bony Pelvis and Lower Limb: Popliteus Muscle. StatPearls. 2023 Jan:(): [PubMed PMID: 30252340]
Smith JM, Varacallo M. Osgood-Schlatter Disease. StatPearls. 2023 Jan:(): [PubMed PMID: 28723024]
Hyland S, Sinkler MA, Varacallo M. Anatomy, Bony Pelvis and Lower Limb: Popliteal Region. StatPearls. 2023 Jan:(): [PubMed PMID: 30422486]
Leib AD, Roshan A, Foris LA, Varacallo M. Baker's Cyst. StatPearls. 2023 Jan:(): [PubMed PMID: 28613525]
Varacallo MA, Mattern P, Acosta J, Toossi N, Denehy KM, Harding SP. Cost Determinants in the 90-Day Management of Isolated Ankle Fractures at a Large Urban Academic Hospital. Journal of orthopaedic trauma. 2018 Jul:32(7):338-343. doi: 10.1097/BOT.0000000000001186. Epub [PubMed PMID: 29738399]
Azam M, Wehrle CJ, Shaw PM. Anatomy, Bony Pelvis and Lower Limb: Tibial Artery. StatPearls. 2023 Jan:(): [PubMed PMID: 30422466]
Garrett A, Geiger Z. Anatomy, Bony Pelvis and Lower Limb: Superficial Peroneal Nerve (Superficial Fibular Nerve). StatPearls. 2023 Jan:(): [PubMed PMID: 30521214]
Lezak B, Massel DH, Varacallo M. Peroneal Nerve Injury. StatPearls. 2023 Jan:(): [PubMed PMID: 31751049]
Torres AL, Ferreira MC. Study of the anatomy of the tibial nerve and its branches in the distal medial leg. Acta ortopedica brasileira. 2012:20(3):157-64. doi: 10.1590/S1413-78522012000300005. Epub [PubMed PMID: 24453596]
Musick SR, Varacallo M. Snapping Hip Syndrome. StatPearls. 2023 Jan:(): [PubMed PMID: 28846235]
Biondi NL, Varacallo M. Anatomy, Bony Pelvis and Lower Limb: Vastus Lateralis Muscle. StatPearls. 2023 Jan:(): [PubMed PMID: 30335342]
Ramage JL, Varacallo M. Anatomy, Bony Pelvis and Lower Limb: Medial Thigh Muscles. StatPearls. 2023 Jan:(): [PubMed PMID: 30521196]
Walters BB, Varacallo M. Anatomy, Bony Pelvis and Lower Limb: Thigh Sartorius Muscle. StatPearls. 2023 Jan:(): [PubMed PMID: 30422484]
Bordoni B, Varacallo M. Anatomy, Bony Pelvis and Lower Limb: Thigh Quadriceps Muscle. StatPearls. 2023 Jan:(): [PubMed PMID: 30020706]
Attum B, Varacallo M. Anatomy, Bony Pelvis and Lower Limb: Thigh Muscles. StatPearls. 2023 Jan:(): [PubMed PMID: 29494052]
Gupton M, Munjal A, Kang M. Anatomy, Bony Pelvis and Lower Limb: Fibula. StatPearls. 2023 Jan:(): [PubMed PMID: 29261984]
Abdel-Hamid MZ, Chang CH, Chan YS, Lo YP, Huang JW, Hsu KY, Wang CJ. Arthroscopic evaluation of soft tissue injuries in tibial plateau fractures: retrospective analysis of 98 cases. Arthroscopy : the journal of arthroscopic & related surgery : official publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 2006 Jun:22(6):669-75 [PubMed PMID: 16762707]
Level 2 (mid-level) evidenceMalik S, Herron T, Mabrouk A, Rosenberg N. Tibial Plateau Fractures. StatPearls. 2023 Jan:(): [PubMed PMID: 29261932]
Varacallo M, Chakravarty R, Denehy K, Star A. Joint perception and patient perceived satisfaction after total hip and knee arthroplasty in the American population. Journal of orthopaedics. 2018 Jun:15(2):495-499. doi: 10.1016/j.jor.2018.03.018. Epub 2018 Mar 30 [PubMed PMID: 29643693]
Varacallo MA, Herzog L, Toossi N, Johanson NA. Ten-Year Trends and Independent Risk Factors for Unplanned Readmission Following Elective Total Joint Arthroplasty at a Large Urban Academic Hospital. The Journal of arthroplasty. 2017 Jun:32(6):1739-1746. doi: 10.1016/j.arth.2016.12.035. Epub 2016 Dec 27 [PubMed PMID: 28153458]
Bourne M, Sinkler MA, Murphy PB. Anatomy, Bony Pelvis and Lower Limb: Tibia. StatPearls. 2023 Jan:(): [PubMed PMID: 30252309]
Beckenkamp PR, Lin CC, Macaskill P, Michaleff ZA, Maher CG, Moseley AM. Diagnostic accuracy of the Ottawa Ankle and Midfoot Rules: a systematic review with meta-analysis. British journal of sports medicine. 2017 Mar:51(6):504-510. doi: 10.1136/bjsports-2016-096858. Epub 2016 Nov 24 [PubMed PMID: 27884861]
Level 1 (high-level) evidenceKokosis G, Schmitz R, Powers DB, Erdmann D. Mandibular Reconstruction Using the Free Vascularized Fibula Graft: An Overview of Different Modifications. Archives of plastic surgery. 2016 Jan:43(1):3-9. doi: 10.5999/aps.2016.43.1.3. Epub 2016 Jan 15 [PubMed PMID: 26848439]
Level 3 (low-level) evidenceVaracallo MA, Fox EJ. Osteoporosis and its complications. The Medical clinics of North America. 2014 Jul:98(4):817-31, xii-xiii. doi: 10.1016/j.mcna.2014.03.007. Epub 2014 May 9 [PubMed PMID: 24994054]
Varacallo MA, Fox EJ, Paul EM, Hassenbein SE, Warlow PM. Patients' response toward an automated orthopedic osteoporosis intervention program. Geriatric orthopaedic surgery & rehabilitation. 2013 Sep:4(3):89-98. doi: 10.1177/2151458513502039. Epub [PubMed PMID: 24319621]
Mostafa E, Imonugo O, Varacallo M. Anatomy, Shoulder and Upper Limb, Humerus. StatPearls. 2023 Jan:(): [PubMed PMID: 30521242]
Jiang LF, Li H, Xin ZF, Wu LD. Computed tomography angiography and magnetic resonance imaging performance of acute segmental single compartment syndrome following an Achilles tendon repair: A case report and literature review. Chinese journal of traumatology = Zhonghua chuang shang za zhi. 2016 Oct 1:19(5):290-294 [PubMed PMID: 27780511]
Level 3 (low-level) evidenceTaube RR, Wadsworth LT, Johnson RJ. Managing Tibial Stress Fractures. The Physician and sportsmedicine. 1993 Apr:21(4):123-30. doi: 10.1080/00913847.1993.11710368. Epub [PubMed PMID: 27447774]
Varacallo M, Shirey L, Kavuri V, Harding S. Acute compartment syndrome of the hand secondary to propofol extravasation. Journal of clinical anesthesia. 2018 Jun:47():1-2. doi: 10.1016/j.jclinane.2018.01.020. Epub 2018 Feb 21 [PubMed PMID: 29476968]
Schmidt AH. Acute compartment syndrome. Injury. 2017 Jun:48 Suppl 1():S22-S25. doi: 10.1016/j.injury.2017.04.024. Epub 2017 Apr 24 [PubMed PMID: 28449851]