Introduction
Papuloerythroderma of Ofuji is a rare skin disorder most commonly found in Japan. It is characterized by polygonal, flat-topped erythematous-brown papules coalescing into sheets that often cover the entire skin surface but spare the skin folds.[1] Papuloerythroderma of Ofuji was first discovered in Japan in 1984 by Ofuji, Furukawa, Miyachi, and Ohno.[2] It is commonly accompanied by pruritus, peripheral eosinophilia, and elevated immunoglobulin E (IgE).[3]
The basis of the disease and initial diagnosis stems from an initial meta-analysis comprised of 170 patients via Torchia et al, who proposed a preliminary set of 5 major and 5 minor criteria that define Papuloerythroderma of Ofuji. These criteria help determine etiology and allow for categorization into 4 subtypes, which include primary, secondary, and a nonpapular form of Papuloerythroderma of Ofuji.[4] There is also a consideration for patients that appear clinically, like Papuloerythroderma of Ofuji, but have a diagnosis more consistent with lymphoma.[5]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Although the underlying etiology of Papuloerythroderma of Ofuji has not been elucidated, a clear connection between underlying malignancy, infectious processes, and pharmacological agents preceding the presentation of Papuloerythroderma of Ofuji has been a consistent theme.[6] The range of oncologic disorders found in association with Papuloerythroderma of Ofuji includes gastric carcinomas, hepatocellular carcinoma, adenocarcinoma of the colon, cutaneous T-cell lymphoma, prostate cancer, and chronic lymphocytic leukemia; however, gastric adenocarcinoma has been noted to be the most common form of malignancy in a meta-analysis of cases of Papuloerythroderma of Ofuji.[1][7][8][9][10] This finding leads to the possibility of Papuloerythroderma of Ofuji being a paraneoplastic syndrome, with screening for underlying malignancy being a crucial component in the work-up of patients with Papuloerythroderma of Ofuji.[11]
In addition to oncologic processes, the hepatitis C virus has also been found to cause Papuloerythroderma of Ofuji, with complete resolution of all lesions after the levels of hepatitis C viral antigen become undetectable.[12] Drug-induced Papuloerythroderma of Ofuji is a distinct T-helper cell type 2 (Th2)-mediated drug hypersensitivity, and the role of Th2 has been implicated in other associated with atopic disease.[3][13] Pharmacological agents associated with this phenomenon include nicardipine, aspirin, isoniazid, furosemide, etretinate, ranitidine, leuprorelin, and diltiazem; interestingly, some of these medications, like etretinate, have been associated with the onset of Papuloerythroderma of Ofuji.[13]
Epidemiology
The incidence of Papuloerythroderma of Ofuji has been reported to be 1.5 cases per million; however, this is considered an underestimate since the condition is likely underdiagnosed.[14] The most common subset of the population affected by Papuloerythroderma of Ofuji consists of those 55 years or older and of Asian or Caucasian descent. There is a predilection for males to females with a ratio of 4 to 1.[1]
Epidemiologic factors, including age and gender, comprise 2 of the 5 minor criteria for diagnosing Papuloerythroderma of Ofuji.[4] The condition is also commonly found in individuals with underlying cutaneous T-cell lymphoma (CTCL).[5][15] This close correlation between the 2 diseases is a common theme and plays a significant role in evaluating Papuloerythroderma of Ofuji.[16]
Pathophysiology
The pathophysiology of Papuloerythroderma of Ofuji remains unclear; however, multiple studies have shown it to be associated with malignancy, medications, infections, and atopic disease, with the resolution of the association generally linked with the cessation of Papuloerythroderma of Ofuji symptoms.[1] For malignancy, there is debate about whether it is a paraneoplastic syndrome since it has been associated with malignancy in between 22% and 55% of cases.[4][9] Because of its association with a strong Th2 response, it has been postulated to arise in relation to atopic disease, allergies, or drug reactions.[17][18][19] Infection has also been postulated as a preceding factor that causes an overactive immune system leading to this condition, but this cause has only been found in 4% of patients.[4][20] Most importantly, because Papuloerythroderma of Ofuji can be conflated with cutaneous lymphoma, particularly CTCL and mycosis fungoides, it has been proposed that its development has to do with an early stage of lymphoma.[5][21]
Histopathology
Histopathological examination of the tissue reveals focal hyperkeratosis and an acanthotic epidermis with some spongiosis.[1] An inflammatory infiltrate is present in a perivascular distribution with a nonspecific collection of plasma cells, eosinophils, macrophages, Langerhans cells, and lymphocytes with rare neutrophils; importantly, lymphocytes can demonstrate exocytosis but do not reveal epidermotropism, which would be more diagnostic for cutaneous lymphoma.[1] These findings are not pathognomonic; however, they aid in diagnosing and evaluating Papuloerythroderma of Ofuji.[10][22]
History and Physical
Included in the history and physical of a patient with suspected Papuloerythroderma of Ofuji, the provider should elucidate the presence of pruritus, establish the status of atopy, and exclude all external triggering factors, including atopy, infectious processes, malignancy (including CTCL), and drug-induced lesions, per the major criteria for diagnosing Papuloerythroderma of Ofuji.[1]
The minor criteria for diagnosing Papuloerythroderma of Ofuji include age over 55, male sex, peripheral eosinophilia, elevated serum IgE, and reduced lymphocyte count.[1][4] A full-body skin examination will likely reveal erythematous lesions comprised of flat, confluent, reddish-brown papules with distribution on the trunk, extremities, and extensor surfaces. In addition to these lesions, a positive deck-chair sign should be present, defined by the exclusion of inframammary folds, axillary folds, inguinal creases, and popliteal fossae.[23] Other findings may include palmoplantar keratoderma and lymphadenopathy, which may raise suspicion of malignancy.[1] Dermoscopy of Papuloerythroderma of Ofuji reveals multiple erythematous pinpoint papules with surrounding whitish halos on an erythematous-pinkish background.[16]
Evaluation
Laboratory, histopathological, and clinical features are the hallmarks of the evaluation of Papuloerythroderma of Ofuji through the major and minor criteria. However, the disease is a diagnosis of exclusion after excluding other causes of erythroderma (eg, atopic dermatitis, psoriasis, malignancy, cutaneous T-cell lymphoma, etc).[1] Laboratory tests, including complete blood count, comprehensive metabolic panel, serum IgE, and titers for Epstein-Barr virus, cytomegalovirus, hepatitis B virus, hepatitis C virus, and HIV should be performed; testing for syphilis, including rapid plasma reagin and venereal diseases reference laboratory tests should be performed.[1]
The presence of lymphopenia, elevated serum IgE, and peripheral eosinophilia are consistent with the diagnosis of Papuloerythroderma of Ofuji.[1] Histological evaluation of a punch biopsy should be performed in patients. Due to the similarity in the clinical presentation of CTCL and that of Papuloerythroderma of Ofuji, patients should undergo flow cytometry and T-cell receptor clonality studies to rule out the possibility of misdiagnosis and to prevent further delay of treatment in patients with CTCL.[5] Further studies have indicated that testing for thymus and activation-regulated chemokine (TARC) may be a diagnostic marker that could help tailor treatment.[1][3] One study suggested obtaining PET scans to rule out malignancy.[1][24][25]
Treatment / Management
Treatment of Papuloerythroderma of Ofuji initially consists of finding the underlying etiology and treating the secondary disease. This step may include the treatment of infectious processes or the removal of pharmacological agents.[1][20] For cases of idiopathic disease, there is no gold standard of therapy; however, cases have been treated with photochemotherapy (psoralen plus ultraviolet A [PUVA]-psoralen and ultraviolet A), topical corticosteroids, methotrexate, azathioprine, interferon alfa, etretinate, and cyclosporine.[1][26][27][28][29][30][31](B3)
Wet wraps and oral antihistamines have been shown as treatments in 2 cases.[32] Additionally, A 9-month course of cyclosporine at 3 mg/kg was noted to lead to complete resolution of skin lesions with some residual postinflammatory change.[13][22] Because of a suggested Th2-based etiology of Papuloerythroderma of Ofuji, newer studies have suggested treatment with dupilumab; however, this may need to be used cautiously after a complete workup for malignancy.[19][33][34][35](A1)
Differential Diagnosis
The differential diagnosis of Papuloerythroderma of Ofuji should include CTCL, secondary syphilis, and drug reaction with eosinophilia and systemic symptoms (DRESS).[1][21][25] CTCL and Papuloerythroderma of Ofuji can be differentiated through flow cytometry and evaluation of clonal T-cell samples; secondary syphilis may be ruled out via VDRL and RPR testing; and DRESS can be differentiated via its acute presentation versus the more gradual, chronic, and indolent course of Papuloerythroderma of Ofuji.[13] There is a wide differential of diseases associated with the deck-chair sign since this is not specific to Papuloerythroderma of Ofuji; the differential can include psoriasis, atopic or contact dermatitis, lymphoma, acanthosis nigricans, and drug eruptions.[1]
Prognosis
The course of Papuloerythroderma of Ofuji is generally indolent, with remission occurring many years after the initial onset in idiopathic cases.[23] Those with secondary etiology leading to Papuloerythroderma of Ofuji may experience rapid clearance of lesions upon removing the offending agents or treating the underlying causes.[1][36] Without secondary bacterial superinfection, the overall disease progression is nonacute and consists of resolving pruritus, which generally leads to complete resolution.[37] It has been noted that the course of Papuloerythroderma of Ofuji is approximately 7 months, but it is expected to be a chronic and indolent skin disease.[1] The association of Papuloerythroderma of Ofuji with atopic disease and malignancy is notable, with one study reporting atopic disease in 20% of patients and reporting malignancy in 22%-55% of patients.[1]
Complications
A significant complication of Papuloerythroderma of Ofuji is secondary bacterial superinfection of the polygonal papular lesions, likely due to excoriation.[1][4] These secondary infections may lead to erysipelas or cellulitis, significantly impacting patients' overall well-being. These complications are manageable with brief oral courses of clindamycin or cefuroxime.[22] In addition to bacterial superinfection, a delay in diagnosis of CTCL can also occur if there is a diagnosis of Papuloerythroderma of Ofuji without proper evaluation to rule out CTCL.[5] It is unclear if lymphoma is an eventual outcome of Papuloerythroderma of Ofuji or if it is a similar diagnosis; for conservative measures, it may be most appropriate to monitor the patient for the development of signs of lymphoma as some have proposed that Papuloerythroderma of Ofuji is a precursor to mycosis fungoides.[1][21][38]
Deterrence and Patient Education
Patients suffering from Papuloerythroderma of Ofuji should receive proper education on the correlations between Papuloerythroderma of Ofuji and multiple internal malignancies, as well as its similarity and possible association with CTCL. Proper screening and evaluation to rule out these internal malignancies are crucial components in the management of Papuloerythroderma of Ofuji, and informing patients regarding the types of screening they should undergo will aid in the adequate evaluation of possible underlying disease processes.
Enhancing Healthcare Team Outcomes
The management of Papuloerythroderma of Ofuji requires the participation of an interprofessional healthcare team approach. Aside from the primary care provider, nurse practitioner, and internist, the involvement of specialists in multiple fields to aid in diagnosing underlying malignancy should have participation at an early stage in the disease process. Pharmacists can be integral in helping determine when the condition is drug-induced, as well as providing recommendations for pharmaceutical therapy. Nursing is often the primary point of contact for patients and families, providing education.
Patients with Papuloerythroderma of Ofuji should undergo evaluation via a gastroenterologist to perform upper endoscopy and colonoscopy to rule out gastric carcinoma and adenocarcinoma of the colon. In addition to proper gastroenterological work-up, patients should be evaluated for any hematological abnormalities and referred to hematology and oncology specialists if any cell line abnormalities, flow cytometry abnormalities, or clinical features of malignancy are present.[7][8][9][10]
Media
(Click Image to Enlarge)
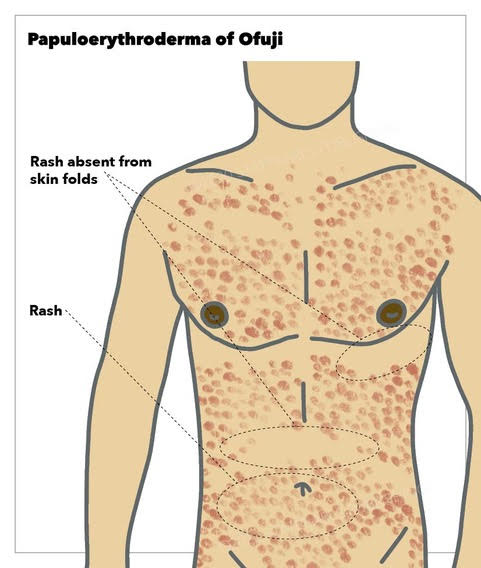
Papuloerythroderma of Ofuji, rash, skin folds StatPearls Publishing Illustration
References
Desai K, Miteva M, Romanelli P. Papuloerythroderma of Ofuji. Clinics in dermatology. 2021 Mar-Apr:39(2):248-255. doi: 10.1016/j.clindermatol.2020.10.017. Epub 2020 Oct 17 [PubMed PMID: 34272018]
Allegue F, Fachal C, González-Vilas D, Zulaica A. Papuloerythroderma of Ofuji successfully treated with methotrexate. Dermatologic therapy. 2018 Jul:31(4):e12638. doi: 10.1111/dth.12638. Epub 2018 Jul 17 [PubMed PMID: 30019369]
Teraki Y, Inoue Y. Skin-homing Th2/Th22 cells in papuloerythroderma of Ofuji. Dermatology (Basel, Switzerland). 2014:228(4):326-31. doi: 10.1159/000358588. Epub 2014 Apr 11 [PubMed PMID: 24732450]
Level 3 (low-level) evidenceTorchia D, Miteva M, Hu S, Cohen C, Romanelli P. Papuloerythroderma 2009: two new cases and systematic review of the worldwide literature 25 years after its identification by Ofuji et al. Dermatology (Basel, Switzerland). 2010:220(4):311-20. doi: 10.1159/000301915. Epub 2010 Mar 26 [PubMed PMID: 20339287]
Level 3 (low-level) evidenceMaher AM, Ward CE, Glassman S, Litvinov IV. The Importance of Excluding Cutaneous T-Cell Lymphomas in Patients with a Working Diagnosis of Papuloerythroderma of Ofuji: A Case Series. Case reports in dermatology. 2018 Jan-Apr:10(1):46-54. doi: 10.1159/000487473. Epub 2018 Feb 21 [PubMed PMID: 29606946]
Level 2 (mid-level) evidenceKhoschbin T, Löser C, Dippel E. [Paraneoplastic skin diseases]. Der Internist. 2019 Aug:60(8):775-782. doi: 10.1007/s00108-019-0636-1. Epub [PubMed PMID: 31273399]
Goto H, Hara H, Takayanagi T, Terui T. Coexistence of papuloerythroderma of Ofuji and acrokeratosis paraneoplastica (Bazex syndrome) preceding the diagnosis of primary hepatocellular carcinoma. International journal of dermatology. 2011 Nov:50(11):1393-1396. doi: 10.1111/j.1365-4632.2010.04852.x. Epub [PubMed PMID: 22004495]
Level 3 (low-level) evidenceSalgüero I, Moreno C, Aguayo-Leiva I, Harto A. Papuloerythroderma of Ofuji associated with chronic lymphatic leukaemia. European journal of dermatology : EJD. 2009 Jul-Aug:19(4):396-7. doi: 10.1684/ejd.2009.0689. Epub 2009 May 25 [PubMed PMID: 19467967]
Level 3 (low-level) evidenceTeraki Y, Aso Y, Sato Y. High incidence of internal malignancy in papuloerythroderma of Ofuji: a case series from Japan. Dermatology (Basel, Switzerland). 2012:224(1):5-9. doi: 10.1159/000335563. Epub 2012 Feb 8 [PubMed PMID: 22327542]
Level 3 (low-level) evidenceSchepers C, Malvehy J, Azón-Masoliver A, Navarra E, Ferrando J, Mascaró JM. Papuloerythroderma of Ofuji: a report of 2 cases including the first European case associated with visceral carcinoma. Dermatology (Basel, Switzerland). 1996:193(2):131-5 [PubMed PMID: 8884150]
Level 3 (low-level) evidenceWick MR, Patterson JW. Cutaneous paraneoplastic syndromes. Seminars in diagnostic pathology. 2019 Jul:36(4):211-228. doi: 10.1053/j.semdp.2019.01.001. Epub 2019 Jan 31 [PubMed PMID: 30736994]
Ota M, Sato-Matsumura KC, Sawamura D, Shimizu H. Papuloerythroderma associated with hepatitis C virus infection. Journal of the American Academy of Dermatology. 2005 Feb:52(2 Suppl 1):61-2 [PubMed PMID: 15692520]
Level 3 (low-level) evidenceSugita K, Kabashima K, Nakamura M, Tokura Y. Drug-induced papuloerythroderma: analysis of T-cell populations and a literature review. Acta dermato-venereologica. 2009 Nov:89(6):618-22. doi: 10.2340/00015555-0712. Epub [PubMed PMID: 19997694]
Level 3 (low-level) evidenceBech-Thomsen N, Thomsen K. Ofuji's papuloerythroderma: a study of 17 cases. Clinical and experimental dermatology. 1998 Mar:23(2):79-83 [PubMed PMID: 9692312]
Level 2 (mid-level) evidenceKim S, Jahan-Tigh R, Duvic M. Papuloerythroderma of Ofuji associated with an indolent CD3(-), CD4(+), TCR(-) peripheral T-cell lymphoma. Leukemia & lymphoma. 2013 Sep:54(9):2059-61. doi: 10.3109/10428194.2012.762976. Epub 2013 Mar 20 [PubMed PMID: 23294328]
Level 3 (low-level) evidenceApalla Z, Koukouthaki A, Sidiropoulos T, Psarakis E, Nikolaidou C, Bobos M, Kampouropoulou E, Lallas A. Dermoscopy of papuloerythroderma of Ofuji. Photodermatology, photoimmunology & photomedicine. 2019 Mar:35(2):127-128. doi: 10.1111/phpp.12441. Epub 2018 Dec 18 [PubMed PMID: 30472755]
Pullmann S, Luger T, Metze D. [Papuloerythroderma of Ofuji with urticarial lesions]. Journal der Deutschen Dermatologischen Gesellschaft = Journal of the German Society of Dermatology : JDDG. 2004 Jun:2(6):443-7 [PubMed PMID: 16281602]
Level 3 (low-level) evidenceCamacho FM, García-Hernandez MJ, Muñoz-Pérez MA, Mazuecos J, Sotillo I. Ofuji papuloerythroderma in an elderly woman with atopic erythroderma. Journal of the European Academy of Dermatology and Venereology : JEADV. 2001 May:15(3):264-6 [PubMed PMID: 11683297]
Level 3 (low-level) evidenceHendricks AJ, Yosipovitch G, Shi VY. Dupilumab use in dermatologic conditions beyond atopic dermatitis - a systematic review. The Journal of dermatological treatment. 2021 Feb:32(1):19-28. doi: 10.1080/09546634.2019.1689227. Epub 2019 Nov 12 [PubMed PMID: 31693426]
Level 1 (high-level) evidenceHasegawa W, Tachibana T, Ito K, Ito M, Toma H, Sato Y. Papuloerythroderma of Ofuji associated with strongyloidiasis. The Journal of dermatology. 2003 Feb:30(2):157-8 [PubMed PMID: 12692386]
Level 3 (low-level) evidenceNashan D, Faulhaber D, Ständer S, Luger TA, Stadler R. Mycosis fungoides: a dermatological masquerader. The British journal of dermatology. 2007 Jan:156(1):1-10 [PubMed PMID: 17199560]
Terlikowska-Brzósko A, Paluchowska E, Owczarek W, Majewski S. Papuloerythroderma of Ofuji in a 41-year-old woman. Postepy dermatologii i alergologii. 2013 Oct:30(5):324-8. doi: 10.5114/pdia.2013.38364. Epub 2013 Oct 30 [PubMed PMID: 24353495]
Level 3 (low-level) evidenceOfuji S, Furukawa F, Miyachi Y, Ohno S. Papuloerythroderma. Dermatologica. 1984:169(3):125-30 [PubMed PMID: 6148269]
Level 3 (low-level) evidenceLee SH, Kim JS, Lee JH, Zheng Z, Cho SB. 18F-fluorodeoxyglucose uptake on positron emission tomography/computed tomography in symmetrically enlarged axillary and inguinal lymph nodes of Ofuji's papuloerythroderma. Leukemia & lymphoma. 2012 Mar:53(3):511-3. doi: 10.3109/10428194.2011.616963. Epub 2011 Oct 24 [PubMed PMID: 21867461]
Level 3 (low-level) evidenceWang D, Chan MMF, Lee HY. Papuloerythroderma of Ofuji presenting as a paraneoplastic phenomenon in myelodysplastic syndrome. The Australasian journal of dermatology. 2018 May:59(2):e155-e156. doi: 10.1111/ajd.12703. Epub 2017 Aug 3 [PubMed PMID: 28771683]
Kasai E, Habe K, Matsushima Y, Kondo M, Yamanaka K. Papuloerythroderma of Ofuji associated with sternoclavicular arthritis and successful treatment with cyclosporine. JAAD case reports. 2022 Sep:27():70-74. doi: 10.1016/j.jdcr.2022.07.004. Epub 2022 Jul 9 [PubMed PMID: 35990234]
Level 3 (low-level) evidenceBalestri R, Magnano M, Rech G, Zorzi MG, Girardelli CR. Long-term use of methotrexate in Papuloerythroderma of Ofuji. Dermatologic therapy. 2020 Mar:33(2):e13219. doi: 10.1111/dth.13219. Epub 2020 Jan 12 [PubMed PMID: 31912936]
Qureshi F, Hughes AJ, Natkunarajah J. Methotrexate for papuloerythroderma of Ofuji. Clinical and experimental dermatology. 2020 Mar:45(2):241-243. doi: 10.1111/ced.13997. Epub 2019 May 21 [PubMed PMID: 31111514]
Quéméneur T, Ghislain PD, Morant C, Devis T, Creuzy C, Modiano P. [Ofuji's papuloerythroderma: two cases treated with azathioprine]. Annales de dermatologie et de venereologie. 2002 Feb:129(2):213-5 [PubMed PMID: 11937960]
Level 3 (low-level) evidenceMutluer S, Yerebakan O, Alpsoy E, Ciftcioglu MA, Yilmaz E. Treatment of papuloerythroderma of Ofuji with Re-PUVA: a case report and review of the therapy. Journal of the European Academy of Dermatology and Venereology : JEADV. 2004 Jul:18(4):480-3 [PubMed PMID: 15196168]
Level 3 (low-level) evidenceFujii K, Kanno Y, Ohgo N. Etretinate therapy for papuloerythroderma. European journal of dermatology : EJD. 1999 Dec:9(8):610-3 [PubMed PMID: 10586126]
Lin L, Chen M, Li L. Wet-wrap therapy combined with compound glycyrrhizin and oral antihistamines as a therapy option for two cases of papuloerythroderma of ofuji. Dermatologic therapy. 2022 Nov:35(11):e15852. doi: 10.1111/dth.15852. Epub 2022 Oct 4 [PubMed PMID: 36153613]
Level 3 (low-level) evidenceKomatsu-Fujii T, Nonoyama S, Ogawa M, Fukumoto T, Tanabe H. Rapid effects of dupilumab treatment on papuloerythroderma of Ofuji. Journal of the European Academy of Dermatology and Venereology : JEADV. 2020 Nov:34(11):e739-e741. doi: 10.1111/jdv.16581. Epub 2020 Jun 26 [PubMed PMID: 32379915]
Teraki Y, Taguchi R, Takamura S, Fukuda T. Use of Dupilumab in the Treatment of Papuloerythroderma of Ofuji. JAMA dermatology. 2019 Aug 1:155(8):979-980. doi: 10.1001/jamadermatol.2019.0946. Epub [PubMed PMID: 31215964]
Schaefer L, Comfere N, Sokumbi O. Development of Cutaneous T-Cell Lymphoma Following Biologic Treatment: A Systematic Review. American journal of clinical dermatology. 2023 Mar:24(2):153-164. doi: 10.1007/s40257-022-00749-1. Epub 2023 Jan 10 [PubMed PMID: 36627479]
Level 1 (high-level) evidenceDwyer CM, Chapman RS, Smith GD. Papuloerythroderma and cutaneous T cell lymphoma. Dermatology (Basel, Switzerland). 1994:188(4):326-8 [PubMed PMID: 8193409]
Level 3 (low-level) evidenceAzón-Masoliver A, Casadó J, Brunet J, Martinez MA, del Castillo D. Ofuji's papuloerythroderma following choledocholithiasis with secondary sepsis: complete resolution with surgery. Clinical and experimental dermatology. 1998 Mar:23(2):84-6 [PubMed PMID: 9692313]
Level 3 (low-level) evidencePatel RH, Fagan K, Chitnavis PV, Grider D. Papuloerythroderma of Ofuji in a Young Man. Cureus. 2023 Mar:15(3):e36598. doi: 10.7759/cureus.36598. Epub 2023 Mar 23 [PubMed PMID: 37095814]