Introduction
Avascular necrosis of the femoral head is a type of osteonecrosis due to disruption of blood supply to the proximal femur. There are approximately 10000 to 20000 new cases reported each year in the United States alone.[1] It can occur due to a variety of causes, either traumatic or atraumatic in origin. These causes include fractures, dislocations, chronic steroid use, chronic alcohol use, coagulopathy, congenital causes; among many others. Avascular necrosis of the femoral head is a debilitating disease and is an important condition requiring healthcare professionals to be vigilant for its presentation. This activity will provide an overview of the etiology and management, along with pertinent clinical pearls.
The majority of the blood supply to the head of the femur comes from the medial and lateral circumflex branches of the profunda femoris, which itself is a branch of the femoral artery (the profunda femoris is the deep penetrating branch of the upper thigh). The medial and lateral circumflex femoral arteries anastomose to form a ring around the neck of the femur, from which many small arteries branch off to perfuse the femoral head. Another direct source of blood supply is from the foveal artery, aka the artery of the ligamentum teres. The ligamentum teres is the ligament connecting the head of the femur to the acetabulum. The foveal artery runs within the ligament, though its contribution is only significant in pediatric populations.[2] Two important anastomoses provide collateral blood flow (though limited) to support the femoral head. One is the cruciate anastomosis, which is between the inferior gluteal artery and the medial circumflex femoral artery. The other is the trochanteric anastomosis, which is between the superior gluteal artery and medial/lateral circumflex femoral arteries. Both the superior and inferior gluteal arteries are branches off of the internal iliac artery (also known as the hypogastric artery) which is the main artery of the pelvis and supplies part of the buttock and posterior thigh.[2] The internal iliac artery comes from the common iliac artery, which in turn comes from the aorta. The femoral head articulates with the acetabulum, which is the “socket” of the hip. The acetabulum’s blood supply comes mainly from the acetabular branch of the obturator artery, along with contributions from pubic branches of the obturator artery, and deep branches of the superior gluteal artery.[3] Because of limited collateral circulation, disruption of the blood supply to the head of the femur can lead to ischemia and subsequent necrosis. If restoration of blood supply does not occur promptly, this will lead to the progressive death of osteocytes followed by the collapse of the articular surface, and eventually by degenerative arthritis.[4]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Many different etiologies can precipitate this condition.
One of the most common traumatic causes is femoral neck fracture or dislocation of the femoral head from acetabulum. When these types of trauma occur, the blood supply to the head of the femur can be easily disrupted, leading to avascular necrosis. Osteonecrosis is the result in 15% to 50% of fractures of the neck of the femur and 10% to 25% of hip dislocations.[5]
Chronic steroid use and excessive alcohol consumption represent the bulk of non-traumatic etiologies, contributing to more than 80% of them. Steroid-associated osteonecrosis represents the second most common cause of osteonecrosis overall, after trauma. Despite evidence demonstrating the correlation between steroid use and osteonecrosis, the exact pathophysiology is not clear and probably multifactorial. The cause is most likely an aggregate of factors such as fat emboli, fat cell hypertrophy leading to increased intraosseous pressure, endothelial dysfunction, hyperlipidemia, and abnormality of the stem cell pool of the bone marrow; all of which contribute to ischemia and subsequent necrosis.[6] Alcohol-induced osteonecrosis is similarly not well understood but most likely stems from bone marrow fat cell hypertrophy and proliferation, serum lipid level changes, blood vessel occlusion, increased intraosseous pressure, and subsequent lack of perfusion.[7]
Sickle cell disease can often precipitate osteonecrosis. The misshapen and rigid red blood cells impede blood flow leading to ischemia and bony infarction, with the femoral head being the most common site of osteonecrosis in these patients.[8] Autoimmune and chronic inflammatory disorders, e.g., systemic lupus erythematosus (SLE), are well-known to be associated with osteonecrosis of the femoral head. The risk of developing the condition in these patients is usually attributed to long-term steroid treatment, though there are reports of cases in those who are steroid naive.[9]
There are other less common, but still clinically important causes, one of which is Legg-Calve-Perthes. Legg-Calve-Perthes is idiopathic avascular necrosis of the femoral head that affects pediatric populations. Lack of blood supply causes necrosis of the femoral head leading to a deformity that puts the patient at high risk of developing osteoarthritis and/or losing range of motion (ROM). This disease progresses through four stages[10][11]:
- Initial/necrosis – when blood supply gets disrupted, and necrosis begins
- Fragmentation – when the body resorbs the necrotic bone and replaces it with woven bone that is weak and prone to breaking and collapse
- Reossification – when stronger bone develops
- Healed/Remodeling – when bone regrowth is complete, and shape becomes finalized (whether normal or abnormal, depending on the damage done during the fragmentation phase)
Vascular disease secondary to diabetes, as well as direct damage from cytotoxic agents have also been implicated in the development of femoral head osteonecrosis.[12]
Epidemiology
The incidence of avascular necrosis of the femoral head within the United States is estimated to occur at a rate between 20000 to 30000 new cases each year, contributing to 10% of the approximately 250000 total hip arthroplasties performed annually.[13] This percentage is comparable to the incidence of 0.01% found in German-speaking countries and the incidence of 1.9 per 100000 found in Japan.[14] There is no association with race, except regarding cases associated with sickle cell disease, which is more prevalent in patients of African descent. Overall, this condition is more prevalent in men than women, with studies estimating ratios from 3 to 1 to 5 to 1.[15][16] The average age at treatment is 33 to 38 years old.[1]
Pathophysiology
The exact pathophysiologic mechanisms behind avascular necrosis of the femoral head are not always clear and generally regarded as being multifactorial.[17] Regardless of the precipitating factor, the outcome is essentially the death of osteocytes and bone marrow that results from insufficient blood flow to the subchondral bone of the proximal femur.[5] This cell death will inevitably lead to a collapse of the femoral head and subsequent osteoarthritis, if not treated effectively in the early stages.
History and Physical
Patients may be asymptomatic early on in the disease process. When they become symptomatic, however, the stated history is usually of hip pain that may radiate to the groin and/or thigh. The pain is typically aggravated by activities such as walking and climbing stairs and alleviated by rest. The pain will often still be present, even in the absence of movement.[17] Some examples of physical exam findings indicative of osteonecrosis of the femoral head are restricted range of motion, pain upon abduction and internal rotation, and tenderness to palpation of the hip region.[18]
Evaluation
Early identification can significantly affect outcomes. Diagnosis is made by pairing the clinical presentation with appropriate imaging. Imaging can include x-rays, radionuclide bone scanning, and magnetic resonance imaging (MRI). The use of imaging in the context of the patient’s symptoms can help guide appropriate treatment.
Plain-film radiography is typically obtained in two planes, utilizing both anterior-posterior and frog-leg lateral films. Radiographs may show subchondral radiolucency, which is the pathognomonic “crescent sign,” indicating subchondral collapse. Uptake of Technetium-99m can show a “donut sign,” which is a ring of increased uptake around a cold center. This sign represents accelerated bone turnover at the demarcation, where reactive bone meets the dead bone.[13] MRI is the gold standard of diagnosis for osteonecrosis. Though both X-rays and radionuclide scans can aid in the diagnosis, neither is as sensitive as MRI; nor as reliable at showing radiographic evidence early in disease progression. MRI can visualize bone marrow changes, size/location of the necrotic area, the effect on acetabular cartilage, depth of collapse, etc.; which are incredibly helpful when ascertaining a patient’s prognosis and formulating a plan of care.[17]
Once obtaining adequate imaging, the extent of necrosis can be classified. While multiple staging systems exist, the most commonly used is the Steinberg staging system. It identifies seven stages as follows:
Steinberg staging system[13]
Stage Features
0 Normal radiograph, bone scan, and MRI
I Normal radiograph, abnormal bone scan and or magnetic resonance imaging
IA Mild (involves less than 15% of the femoral head).
IB Moderate (involves 15% to 30% of the femoral head)
IC Severe (involves over 30% of the femoral head)
II Cystic and sclerotic change of the femoral head
IIA Mild (involves less than 15% of the femoral head)
IIB Moderate (involves 15% to 30% of the femoral head)
IIC Severe (involves more than than 30% of the femoral head)
III Subchondral collapse (crescent sign) without flattening of the femoral head
IIIA Mild (involves under 15% of the femoral head)
IIIB Moderate (involves 15% to 30% of the femoral head)
IIIC Severe (involves over 30% of the femoral head)
IV Flattening of the femoral head/femoral head collapse
IVA Mild (involves under 15% of the femoral head)
IVB Moderate (involves 15% to 30% of the femoral head)
IVC Severe (involves greater than 30% of the femoral head)
V Joint space narrowing and/or acetabular changes
VA Mild
VB Moderate
VC Severe
VI Advanced degenerative joint disease
A laboratory workup should be done to help rule out other causes of hip pain as well as to assess for comorbid factors in patients with suspected osteonecrosis. A workup may include a complete blood count (CBC), lipid panel, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), rheumatoid factor (RF), anti-nuclear antibody (ANA), anti-cyclic citrullinated peptide (anti-CCP), and hemoglobin electrophoresis. Elevated ANA and/or RF would indicate an active autoimmune process but are non-specific. Both ESR and CRP are elevated by inflammatory processes but are also non-specific. Elevated anti-CCP antibodies are specific for rheumatoid arthritis, while hemoglobin electrophoresis showing HbS with a low concentration of HbF would indicate sickle cell disease.[19][20] A CBC showing evidence of normocytic or microcytic anemia with an elevated reticulocyte count would also be consistent with a diagnosis of sickle cell disease. Rheumatoid arthritis and sickle cell disease are two conditions that can precipitate the development of osteonecrosis in the femoral head and can cause hip pain even without osteonecrosis.
A biopsy is not often necessary, as the diagnosis can be made accurately based off imaging and clinical presentation. If a biopsy is performed, however, the characteristic histological findings will be trabecular necrosis (more than 50% of empty osteocytic lacunae) and necrotic hematopoietic marrow without specific evidence of inflammation, tumor cells, or sepsis.[21] Similarly, angiography studies are not routinely performed, though they do provide good visualization of the vasculature and may contribute to research and understanding of disease pathology.[22][19]
Treatment / Management
The management of avascular necrosis of the femoral head ranges from conservative to invasive. The exact therapy utilized is dependent upon many factors, and each patient must have their case evaluated individually for optimization. Such factors include the age of the patient, level of pain/discomfort, location and extent of necrosis, comorbidities, and of course, whether the collapse of the articular surface has occurred or not. Treatments are best implemented at the pre-collapse stage and include both operatives as well as non-operatives options. If left untreated, femoral head necrosis may lead to subchondral fractures within only 2 to 3 years.[17][23]
Treatment decisions should be based on the staging of the lesions but mainly on the presence or absence of collapse. Generally, non-operative treatments or core decompression can show value in asymptomatic and symptomatic small to medium-sized pre-collapse lesions. Medium to larger-sized lesions can have treatment with bone grafting (vascularized or non-vascularized), or osteotomies. If femoral collapse has occurred or acetabular involvement is present, arthroplasty is indicated.
Conservative management spans a variety of non-operative treatments. These may include physical therapy, restricted weight-bearing, alcohol cessation, discontinuation of steroid therapy, pain control medication, and targeted pharmacologic therapy, among others. Since avascular necrosis of the femoral head shows a marked variation in the time to progression and/or collapse, and evidence is scarce; there is no agreement on conservative treatments. Despite small asymptomatic lesions being able to resolve spontaneously, most progress and require treatment. Vasodilators, statins, bisphosphonates, and anticoagulants have been used off-label in an attempt to revascularize the femoral head. Vasodilators, including iloprost (PGI2), are intended to decrease intraosseous pressure, allowing for increased blood flow.[24] Statins act to decrease the differentiation of stem cells into fat cells, again intending to decrease intraosseous pressure for better perfusion.[25] Anticoagulants, such as enoxaparin are used to prevent the progression of osteonecrosis due to hypercoagulability and thromboembolic events.[26] Bisphosphonates, including alendronate, inhibit the action of osteoclasts from decreasing bone resorption.[27][28] Despite the variety of options available for pharmacologic treatment, there currently is not a strong consensus on the effectiveness of any one of these agents over another. Intra-articular steroid injections are generally not recommended at all. Although they may provide pain relief, the effects are usually short-lived, and their use can cause significant worsening of avascular necrosis.[29] (A1)
There are several surgical options for those who require more invasive treatment. They fall into categories as either joint preservative or joint reconstructive procedures. The joint preservation interventions include core decompression, bone grafts, use of biologics and/or cellular therapies, and osteotomy; while reconstructive interventions entail a joint replacement.
Core decompression is the surgical removal (via drilling) of affected tissue from the inside the femoral head to decrease pressure and increase perfusion and is the most common intervention during pre-collapse stages. Cell-therapies have been used as adjuvants to core decompression and have been reported to be safe and suggest improved clinical outcomes with lower disease progression rate than core decompression alone.[30][31][32] Overall, core decompression has shown good outcomes and is a good option for symptomatic small to medium-sized precollapse lesions; however, it is not indicated when the femoral head has collapsed. (A1)
Bone grafting is an alternative to treatment of larger size lesions with no early collapse. A bone graft can be taken from another part of the patient’s own body (autograft), from another part of the patient’s own body along with intact vasculature (vascularized bone graft), or another person via a bone bank (allograft). The vascularized bone graft has the added value of carrying a new blood supply that can improve the revascularization of the bone and potentially revitalize the necrotic zone. Osteotomy is the removal of portions of bone to alter the weight distribution of the joint to the healthy, uninvolved bone. These procedures usually include rotational trans-trochanteric or angular intertrochanteric procedures, in which the necrotic region of the femoral head can be moved away from weight-bearing regions, theoretically allowing healing or delaying progression.[33]
If the damage is extensive, the collapse has occurred, and/or there is acetabular involvement; then arthroplasty may be required; this involves the removal of the ball-and-socket of the hip and replacement with a prosthetic.[13] While previously demonstrating mixed success rates, in the past twenty years there have been improvements in hardware such as surface bearings with low wear rates that have significantly improved the outcome of hip replacement in the setting of osteonecrosis.[34][17]
Differential Diagnosis
Symptoms of avascular necrosis of the femoral head overlap with other etiologies that are important to include in a differential diagnosis. One is bone marrow edema syndrome (BMES), aka transient osteoporosis, that usually occurs as a reactive response to an injury, increases in physical activity, or to osteoarthritis. This condition presents as rapid-onset, sometimes atraumatic, hip pain that is self-limited and typically resolves within one year. MRI is usually significant for widespread bone marrow edema, which gives the disease its eponymous title.[35] Another condition that can become confused for osteonecrosis of the proximal head of the femur is a subchondral fracture, which usually occurs as a fracture after minor trauma in the elderly, in the context of osteoporosis leading to subchondral insufficiency.
Problems to consider in the differential include the following:
- Complex regional pain syndrome
- Inflammatory synovitis
- Neoplastic bone conditions
- Osteomyelitis
- Osteoarthritis
- Osteoporosis
- Soft tissue trauma
Prognosis
The prognosis of femoral head osteonecrosis is dependent upon many factors. One is the point in which it gets diagnosed. The earlier in the disease process the diagnosis occurs, the more effective the preemptive measures, and the better the prognosis. In addition to advanced disease at the time of diagnosis, some other indicators of a poor prognosis include lateral head involvement (as opposed to medial), the involvement of greater than one-third of the weight-bearing portion of the femoral head (as determined by MRI), and age greater than 50-years-old[36]. Even with the presence of one or more of these factors, a patient’s prognosis can vary and should be determined by a qualified physician after appropriate evaluation.[37]
Complications
Complications include progressively worsening joint pain, restricted range of motion, and osteoarthritis.[38] These complications can cause significant disability in patients.
Consultations
When a clinician suspects a patient of having osteonecrosis of the femoral head, consultation from a qualified orthopedic surgeon is for expert evaluation.
Deterrence and Patient Education
Patients should seek medical care if they are experiencing pain in the hip, thighs, and/or buttocks. Also, certain patient populations should be advised of the risk factors and screened as needed; since early avascular necrosis of the femoral head can be asymptomatic. Examples of higher-risk patients include those on long-term steroid treatment, long-term bisphosphonates, excessive alcohol use, hemoglobinopathies, chemotherapy or radiation patients, and those who suffer trauma to the hip and surrounding area.[13]
Enhancing Healthcare Team Outcomes
Healthcare teams are often made up of many interprofessional members and can include (but are not limited to) a physician, nurse practitioner or physician assistant, pharmacist, and nurse. All such team members treating patients with avascular necrosis of the femoral head must be able to not only recognize the condition but also to participate in a competent management plan and obtain expert consultation when indicated. The pharmacist can help with assessing medication regimens, both leading up to AVN as well as attempts to treat AVN pharmaceutically, reporting any concerns to the physician.
If the patient requires surgery, an orthopedic specialist will lead the treatment, and nursing will assist in preparing the patient for surgery, monitor the patient during and after surgery, and check on treatment efficacy as well as administer post-operative medications, with an eye towards watching for adverse effects, which should be reported promptly.
The primary care clinicians, including nurses, should educate patients about the harms of alcohol. Also, clinicians should prescribe the lowest effective dose of corticosteroids. Nursing and physicians should ask patients on long term corticosteroids should be asked about hip symptoms at every clinic visit. The pharmacist should provide patient education on the necessity to quit smoking and can work with the physician on pharmaceutical aids to assist with smoking cessation. Patients should receive training about the symptoms of AVN so that they can seek help early.
Improved awareness and knowledge of avascular necrosis of the femoral head for each interprofessional healthcare team member will improve patient care and prognostic outcomes. [Level V]
Media
(Click Image to Enlarge)
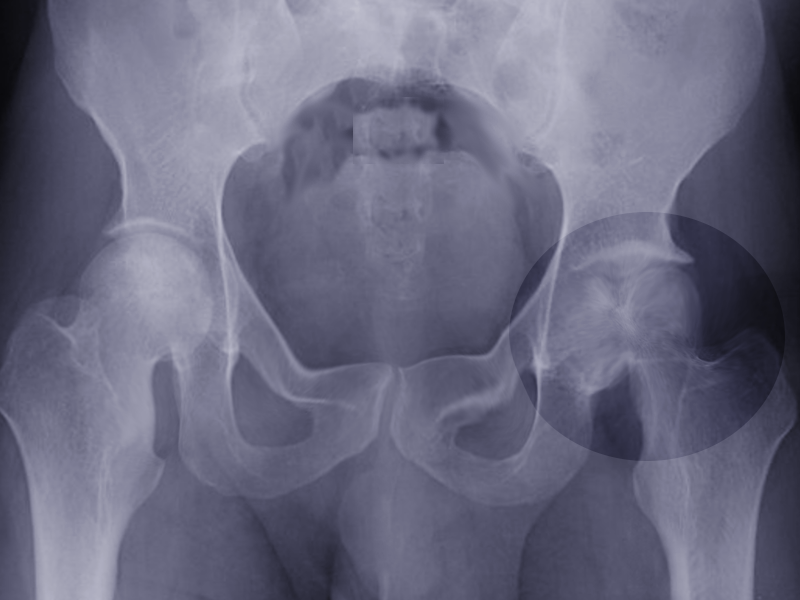
Severe AVN of hip Image courtesy S Bhimji
(Click Image to Enlarge)

Dysbaric Osteonecrosis of the Hip
Contributed by UHM 2005, Vol. 32, No. 3 – Dysbaric osteonecrosis by X-ray and CT scan in Chinese divers. JIANG et al
References
Petek D, Hannouche D, Suva D. Osteonecrosis of the femoral head: pathophysiology and current concepts of treatment. EFORT open reviews. 2019 Mar:4(3):85-97. doi: 10.1302/2058-5241.4.180036. Epub 2019 Mar 15 [PubMed PMID: 30993010]
Gold M, Munjal A, Varacallo M. Anatomy, Bony Pelvis and Lower Limb, Hip Joint. StatPearls. 2024 Jan:(): [PubMed PMID: 29262200]
Itokazu M, Takahashi K, Matsunaga T, Hayakawa D, Emura S, Isono H, Shoumura S. A study of the arterial supply of the human acetabulum using a corrosion casting method. Clinical anatomy (New York, N.Y.). 1997:10(2):77-81 [PubMed PMID: 9058012]
Narayanan A, Khanchandani P, Borkar RM, Ambati CR, Roy A, Han X, Bhoskar RN, Ragampeta S, Gannon F, Mysorekar V, Karanam B, V SM, Sivaramakrishnan V. Avascular Necrosis of Femoral Head: A Metabolomic, Biophysical, Biochemical, Electron Microscopic and Histopathological Characterization. Scientific reports. 2017 Sep 6:7(1):10721. doi: 10.1038/s41598-017-10817-w. Epub 2017 Sep 6 [PubMed PMID: 28878383]
Baig SA, Baig MN. Osteonecrosis of the Femoral Head: Etiology, Investigations, and Management. Cureus. 2018 Aug 21:10(8):e3171. doi: 10.7759/cureus.3171. Epub 2018 Aug 21 [PubMed PMID: 30357068]
Xie XH, Wang XL, Yang HL, Zhao DW, Qin L. Steroid-associated osteonecrosis: Epidemiology, pathophysiology, animal model, prevention, and potential treatments (an overview). Journal of orthopaedic translation. 2015 Apr:3(2):58-70. doi: 10.1016/j.jot.2014.12.002. Epub 2015 Jan 13 [PubMed PMID: 30035041]
Level 2 (mid-level) evidenceJaffré C, Rochefort GY. Alcohol-induced osteonecrosis--dose and duration effects. International journal of experimental pathology. 2012 Feb:93(1):78-9; author reply 79. doi: 10.1111/j.1365-2613.2011.00798_1.x. Epub [PubMed PMID: 22264288]
Level 3 (low-level) evidenceAdesina O, Brunson A, Keegan THM, Wun T. Osteonecrosis of the femoral head in sickle cell disease: prevalence, comorbidities, and surgical outcomes in California. Blood advances. 2017 Jul 11:1(16):1287-1295. doi: 10.1182/bloodadvances.2017005256. Epub 2017 Jul 11 [PubMed PMID: 29296770]
Level 3 (low-level) evidenceMok MY, Farewell VT, Isenberg DA. Risk factors for avascular necrosis of bone in patients with systemic lupus erythematosus: is there a role for antiphospholipid antibodies? Annals of the rheumatic diseases. 2000 Jun:59(6):462-7 [PubMed PMID: 10834864]
Level 2 (mid-level) evidenceMills S, Burroughs KE. Legg-Calve-Perthes Disease. StatPearls. 2024 Jan:(): [PubMed PMID: 30020602]
Rampal V, Clément JL, Solla F. Legg-Calvé-Perthes disease: classifications and prognostic factors. Clinical cases in mineral and bone metabolism : the official journal of the Italian Society of Osteoporosis, Mineral Metabolism, and Skeletal Diseases. 2017 Jan-Apr:14(1):74-82. doi: 10.11138/ccmbm/2017.14.1.074. Epub 2017 May 30 [PubMed PMID: 28740529]
Level 3 (low-level) evidenceTripathy SK, Goyal T, Sen RK. Management of femoral head osteonecrosis: Current concepts. Indian journal of orthopaedics. 2015 Jan-Feb:49(1):28-45. doi: 10.4103/0019-5413.143911. Epub [PubMed PMID: 25593355]
Moya-Angeler J, Gianakos AL, Villa JC, Ni A, Lane JM. Current concepts on osteonecrosis of the femoral head. World journal of orthopedics. 2015 Sep 18:6(8):590-601. doi: 10.5312/wjo.v6.i8.590. Epub 2015 Sep 18 [PubMed PMID: 26396935]
Hofmann S, Kramer J, Plenk H. [Osteonecrosis of the hip in adults]. Der Orthopade. 2005 Feb:34(2):171-83; quiz 184 [PubMed PMID: 15714357]
Ikeuchi K, Hasegawa Y, Seki T, Takegami Y, Amano T, Ishiguro N. Epidemiology of nontraumatic osteonecrosis of the femoral head in Japan. Modern rheumatology. 2015 Mar:25(2):278-81. doi: 10.3109/14397595.2014.932038. Epub 2014 Jul 18 [PubMed PMID: 25036228]
Vardhan H, Tripathy SK, Sen RK, Aggarwal S, Goyal T. Epidemiological Profile of Femoral Head Osteonecrosis in the North Indian Population. Indian journal of orthopaedics. 2018 Mar-Apr:52(2):140-146. doi: 10.4103/ortho.IJOrtho_292_16. Epub [PubMed PMID: 29576641]
Level 2 (mid-level) evidenceArbab D, König DP. Atraumatic Femoral Head Necrosis in Adults. Deutsches Arzteblatt international. 2016 Jan 22:113(3):31-8. doi: 10.3238/arztebl.2016.0031. Epub [PubMed PMID: 26857510]
Karim R, Goel KD. Avascular necrosis of the hip in a 41-year-old male: a case study. The Journal of the Canadian Chiropractic Association. 2004 Jun:48(2):137-41 [PubMed PMID: 17549225]
Level 3 (low-level) evidenceMangla A, Ehsan M, Agarwal N, Maruvada S. Sickle Cell Anemia. StatPearls. 2024 Jan:(): [PubMed PMID: 29489205]
Zabinski SJ, Sculco TP, Dicarlo EF, Rivelis M. Osteonecrosis in the rheumatoid femoral head. The Journal of rheumatology. 1998 Sep:25(9):1674-80 [PubMed PMID: 9733445]
Level 2 (mid-level) evidenceMukisi-Mukaza M, Gomez-Brouchet A, Donkerwolcke M, Hinsenkamp M, Burny F. Histopathology of aseptic necrosis of the femoral head in sickle cell disease. International orthopaedics. 2011 Aug:35(8):1145-50. doi: 10.1007/s00264-010-1121-6. Epub 2010 Sep 10 [PubMed PMID: 20830473]
Zlotorowicz M, Czubak J, Kozinski P, Boguslawska-Walecka R. Imaging the vascularisation of the femoral head by CT angiography. The Journal of bone and joint surgery. British volume. 2012 Sep:94(9):1176-9. doi: 10.1302/0301-620X.94B9.29494. Epub [PubMed PMID: 22933487]
Hsu H, Nallamothu SV. Hip Osteonecrosis. StatPearls. 2024 Jan:(): [PubMed PMID: 29763129]
Claßen T, Becker A, Landgraeber S, Haversath M, Li X, Zilkens C, Krauspe R, Jäger M. Long-term Clinical Results after Iloprost Treatment for Bone Marrow Edema and Avascular Necrosis. Orthopedic reviews. 2016 Mar 21:8(1):6150. doi: 10.4081/or.2016.6150. Epub 2016 Mar 31 [PubMed PMID: 27114807]
Pritchett JW. Statin therapy decreases the risk of osteonecrosis in patients receiving steroids. Clinical orthopaedics and related research. 2001 May:(386):173-8 [PubMed PMID: 11347831]
Level 2 (mid-level) evidenceGlueck CJ, Freiberg RA, Sieve L, Wang P. Enoxaparin prevents progression of stages I and II osteonecrosis of the hip. Clinical orthopaedics and related research. 2005 Jun:(435):164-70 [PubMed PMID: 15930934]
Level 3 (low-level) evidenceLai KA, Shen WJ, Yang CY, Shao CJ, Hsu JT, Lin RM. The use of alendronate to prevent early collapse of the femoral head in patients with nontraumatic osteonecrosis. A randomized clinical study. The Journal of bone and joint surgery. American volume. 2005 Oct:87(10):2155-9 [PubMed PMID: 16203877]
Level 1 (high-level) evidenceAgarwala S, Shah S, Joshi VR. The use of alendronate in the treatment of avascular necrosis of the femoral head: follow-up to eight years. The Journal of bone and joint surgery. British volume. 2009 Aug:91(8):1013-8. doi: 10.1302/0301-620X.91B8.21518. Epub [PubMed PMID: 19651826]
Immonen I, Friberg K, Grönhagen-Riska C, von Willebrand E, Fyhrquist F. Angiotensin-converting enzyme in sarcoid and chalazion granulomas of the conjunctiva. Acta ophthalmologica. 1986 Oct:64(5):519-21 [PubMed PMID: 3028032]
Piuzzi NS, Chahla J, Schrock JB, LaPrade RF, Pascual-Garrido C, Mont MA, Muschler GF. Evidence for the Use of Cell-Based Therapy for the Treatment of Osteonecrosis of the Femoral Head: A Systematic Review of the Literature. The Journal of arthroplasty. 2017 May:32(5):1698-1708. doi: 10.1016/j.arth.2016.12.049. Epub 2017 Jan 12 [PubMed PMID: 28162838]
Level 1 (high-level) evidenceChughtai M, Piuzzi NS, Khlopas A, Jones LC, Goodman SB, Mont MA. An evidence-based guide to the treatment of osteonecrosis of the femoral head. The bone & joint journal. 2017 Oct:99-B(10):1267-1279. doi: 10.1302/0301-620X.99B10.BJJ-2017-0233.R2. Epub [PubMed PMID: 28963146]
Piuzzi NS, Chahla J, Jiandong H, Chughtai M, LaPrade RF, Mont MA, Muschler GF, Pascual-Garrido C. Analysis of Cell Therapies Used in Clinical Trials for the Treatment of Osteonecrosis of the Femoral Head: A Systematic Review of the Literature. The Journal of arthroplasty. 2017 Aug:32(8):2612-2618. doi: 10.1016/j.arth.2017.02.075. Epub 2017 Mar 15 [PubMed PMID: 28392136]
Level 1 (high-level) evidenceLespasio MJ, Sodhi N, Mont MA. Osteonecrosis of the Hip: A Primer. The Permanente journal. 2019:23():. pii: 18-100. doi: 10.7812/TPP/18-100. Epub [PubMed PMID: 30939270]
Kim YH, Kim JS, Park JW, Joo JH. Contemporary total hip arthroplasty with and without cement in patients with osteonecrosis of the femoral head: a concise follow-up, at an average of seventeen years, of a previous report. The Journal of bone and joint surgery. American volume. 2011 Oct 5:93(19):1806-10. doi: 10.2106/JBJS.J.01312. Epub [PubMed PMID: 22005866]
Choi HR, Steinberg ME, Y Cheng E. Osteonecrosis of the femoral head: diagnosis and classification systems. Current reviews in musculoskeletal medicine. 2015 Sep:8(3):210-20. doi: 10.1007/s12178-015-9278-7. Epub [PubMed PMID: 26088795]
Goker B, Block JA. Risk of contralateral avascular necrosis (AVN) after total hip arthroplasty (THA) for non-traumatic AVN. Rheumatology international. 2006 Jan:26(3):215-9 [PubMed PMID: 15761731]
Level 2 (mid-level) evidenceNiimi R, Sudo A, Hasegawa M, Uchida A. Course of avascular necrosis of femoral head without collapse of femoral head at first examination: minimum 8-year follow-up. Orthopedics. 2008 Aug:31(8):755 [PubMed PMID: 19292420]
Hauzeur JP, De Maertelaer V, Baudoux E, Malaise M, Beguin Y, Gangji V. Inefficacy of autologous bone marrow concentrate in stage three osteonecrosis: a randomized controlled double-blind trial. International orthopaedics. 2018 Jul:42(7):1429-1435. doi: 10.1007/s00264-017-3650-8. Epub 2017 Oct 7 [PubMed PMID: 28988340]
Level 1 (high-level) evidence