Introduction
The left atrial appendage (LAA) is a unique structure within the pericardium, close to the free wall of the left ventricle. It has unique developmental, structural, and physiological characteristics that separate it from the left atrium proper.[1] In normal cardiac physiology, the LAA plays an essential role in regulating intravascular volume by releasing natriuretic peptides in response to hemodynamic changes. The LAA also plays a vital role in the pathogenesis of transient ischemic attack (TIA) and stroke in patients with atrial fibrillation (AF).[2]
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The left atrial appendage is often described as a small ear-shaped outpouching of the muscular wall of the left atrium. It lies anteriorly in the atrioventricular sulcus, close to the left circumflex artery, phrenic nerve, and pulmonary veins.[3][4] It is adjacent to the free wall of the left ventricle and, thus, is closely associated with left ventricular function. Although several physiological variants exist, in most individuals, the LAA is a unilobar structure lying parallel to the left superior pulmonary vein. A structural analysis of the LAA using computerized tomography (CT) in 612 individuals suggested that, on average, the appendage is 46 mm long and has a volume of approximately 9 mL.[2] The most common general topology of the LAA is for it to project anterosuperiorly to lie over the superior-most part of the left ventricle or the pulmonary trunk. In a small number of cases, it may be pointed behind the pulmonary trunk directly in the transverse cardiac sinus.[5] The interior surface of the LAA is muscular and marked with muscular ridges, in contrast to the rest of the left atrial interior surface, which is smooth, a difference that can be explained by their embryological origins, as described later.
In normal cardiac physiology, the LAA is an essential modulator of intravascular volume. In response to increased myocyte stretch, the LAA releases atrial natriuretic peptide (ANP) and brain natriuretic peptide (BNP) into the coronary sinus. From here, these peptides enter the general circulation and regulate blood pressure and volume via their diuretic, natriuretic, and vasodilatory effects.[6] The action of ANP in response to increased myocyte stretch includes changes in both renal and systemic vasculature function. ANP promotes acute increased glomerular filtration and thus renal excretion of sodium and water.[7] Furthermore, its effect on the vasculature includes vascular smooth muscle relaxation and increased microvasculature permeability, which promotes protein movement into the interstitial space, effectively decreasing circulating intravascular volume. BNP is stored in a significantly lower concentration in the LAA compared to ANP and is found in greater concentration in the cardiac ventricles.[8][9] Nevertheless, it is also released from the LAA in response to cardiac overload. It is a sensitive biomarker for heart failure, as its levels rise markedly in response to congestive heart failure. BNP's half-life is around 20 minutes, significantly longer than that of ANP, which is approximately only 2 minutes.[10]
Embryology
The left atrial appendage develops during the fourth week of embryonic development as a remnant of the embryonic left atrium (LA), which forms during the third week of gestation.[1][11] This development contrasts with the rest of the LA cavity, which develops as an outgrowth of the pulmonary veins.[12] For this reason, the LAA is marked with muscular ridges in contrast to the rest of the left atrium, which is smooth-walled.
Nerves
The left atrial appendage does not have significant nervous innervation.
Muscles
The left atrial appendage does not perfuse any muscles.
Physiologic Variants
There are several well-described left atrial appendage morphologies. The LAA classification system has its basis on the shape, the relationship of the LAA to the left superior pulmonary vein, length from the ostium to apex, number of lobes, angle of the fist bend formed by the primary lobe, and the distance from the first bend to the LAA orifice. Based on these features, Wang et. described four classical structural morphologies accounting for the majority of anatomical variants seen.[2]
The “chicken wing” morphology describes an LAA with an obvious bend in the proximal or middle part of the dominant lobe and is the most common variant found in one study of 932 patients to be present in 40%.[3] The “cactus” LAA has a dominant central lobe with secondary lobes extending from the central lobe in both superior and inferior directions and was found in 30% of patients. The “windsock” morphology describes an LAA in which one dominant lobe of sufficient length is the primary structure, found in 19% of patients. Finally, the “cauliflower” LAA’s main characteristic is an LAA that has limited overall length with complex internal features, present in just 3% of patients.
Surgical Considerations
In open cardiac procedures, such as coronary artery bypass grafts (CABG), the left atrial appendage is often isolated or ligated. This process is especially important in patients with a history of AF, as isolation and catheter ablation correlates with a decrease in AF recurrence and a reduction in stroke risk.[13] The 2021 Left Atrial Appendage Occlusion Study (LAAOS III) was a randomized control trial treating patients undergoing cardiac surgery who had atrial fibrillation and a stroke risk score (CHA2DS2-VASC) of two or more with either standard of care or LAA occlusion at the time of their cardiac surgery.[14][15][14] The rationale behind this was that these patients are at increased risk of ischemic stroke as implied by their CHA2DS2-VASc score, and given the significant morbidity and mortality from ischaemic stroke, the known pathogenic site of LAA, and the relatively simple procedure for occlusion during concomitant cardiac surgery for other pathology, this may provide a good opportunity to administer prophylactic intervention in this patient group. The results of this trial, which included 4811 patients, demonstrated that in the intervention group undergoing concomitant LAA occlusion at the time of cardiac surgery, there was a 33% reduced risk of ischaemic stroke compared to the group undergoing cardiac surgery only.[16]
Furthermore, the addition of LAA occlusion added no significant extra time to heart bypass during the concomitant procedure being performed. Despite removing the proposed source of embolic stroke from circulation, the authors did not recommend ceasing therapeutic anticoagulation following LAA occlusion, given the lack of evidence comparing LAA occlusion alone versus anticoagulation for stroke prevention. Interestingly, despite a hypothesized increase in heart failure one might observe in patients following LAA occlusion owing to the physiologically impaired ability to excrete sodium and water in volume overload from reduced atrial natriuretic peptide production, there was no statistical difference in the incidence of heart failure between the groups in LAAOS III, either immediately post-operatively or at long-term follow-up.[17][14]
Although providing solid evidence for the use of LAA in the cardiac surgery setting for patients with atrial fibrillation, there remains a question as to the best way to manage ischaemic stroke risk in patients with atrial fibrillation who do not have cardiac surgery planned. Any surgical intervention carries risk, and randomized control trials are needed to interrogate the relative benefit of continuing anticoagulation alone or undertaking LAA occlusion in patients with atrial fibrillation with no cardiac surgery planned.[16] Of note, although studies such as the PROTECT-AF and PREVAIL clinical trials have compared the use of the Watchman LAA closure device with anticoagulation with warfarin only, the recent ascent of the use of direct-acting oral anticoagulants (DOACs) for a broad range of indications including atrial fibrillation means that these trials need to be updated with a direct comparison of these new drugs (e.g., apixaban, rivaroxaban, dabigatran) in order to be relevant to the current population.[18][19][18][20] However, existing evidence regarding the risk of left atrial appendage occlusion devices shows there are several known associated complications, including hematoma associated with vascular access, air embolism related to device-delivery sheaths, and pericardial effusion associated with the transseptal puncture approach for device implantation, and the relative risk of these must be examined in the context of the anticoagulated atrial fibrillation patient group.[21]
Clinical Significance
The LAA is implicated in the pathogenesis of several conditions, including AF and hypertension.
It is well established that the LAA is the primary site of thrombi formation in patients with nonvalvular AF.[2] Researchers postulate that the LAA is the source of thromboembolism in up to 90% of these patients[22]. In normal sinus rhythm, there is good blood flow within the LAA and thus no thrombus formation in normal cardiac function. However, in atrial fibrillation there is reduced contractility, flow stasis, and this consequently causes the LAA to act more as a static pouch in which thombi can easily form[5]. Therefore, anticoagulation therapy and/or LAA occlusion systems are often used prophylactically to reduce stroke risk in these patients. Until recently, there has been little published data on the impact that LAA isolation has on the release of ANP. Several animal models demonstrated an immediate reduction in the immediate levels of ANP secretion following an atrial appendectomy.[6] However, these studies did not explore the long-term effects on ANP levels associated with the isolation of the LAA.
The 2018 LAA HOMEOSTASIS study was one of the first studies which examined the impact of epicardial and endocardial LAA occlusion techniques on neurohormonal modulation in humans. This study, consisting of 77 patients, found that after epicardial LAA closure, ANP and BNP levels decrease significantly immediately post-procedure, began to rise at 24 hours, and normalized at three months. In patients undergoing endocardial LAA device implantations, the ANP/BNP levels significantly increased post-procedure and normalized by three months. Of note, epicardial LAA devices were associated with a down-regulation of the adrenergic system and RAAS, resulting in a significant decrease in systolic blood pressure. No such effect was noted in endocardial device implantations.[23] Further studies are required to determine what effect, if any, these changes in neurohormonal regulation may have on outcomes or patient management.
LAA morphology has demonstrated a correlation with the risk of stroke in patients with atrial fibrillation. Following large imaging cohorts of patients, four main LAA morphologies have been classified: chicken wing, cactus, windsock, and califlower - the former of these four being the most prevelant found in 48% of patients and the other found in 30%, 19%, and 3%, respectively[24]. A multicenter study found that in patients with AF, the cauliflower morphology was associated with the highest risk of stroke, while those with the chicken wing morphology had the lowest risk of stroke.[3] This consideration may be a valuable consideration when developing a more sophisticated risk assessment for the chronic management of individuals with AF.
There have also been reports of tears in the LAA associated with blunt chest wall trauma from motor vehicle accidents. Despite being a rare complication, these injuries correlate with high morbidity and mortality. Approximately 10% of blunt trauma to the chest involves the LAA, and mortality estimates range between 50% to 80%.[25] There are multiple causes for cardiac rupture, ranging from simple blows to severe directional forces. The heart is particularly vulnerable as it hangs freely in the mediastinum, suspended by the great vessels between the sternum and thoracic vertebrae.[26] All chambers of the heart are susceptible to injury, but the LAA is particularly vulnerable due to its relative thinness. The presence of an intact pericardium is a protective factor in these injuries—restricting the effects of tamponade, thereby preventing fatal exsanguination and allowing for patients to survive the journey to the hospital.[25]
Media
(Click Image to Enlarge)
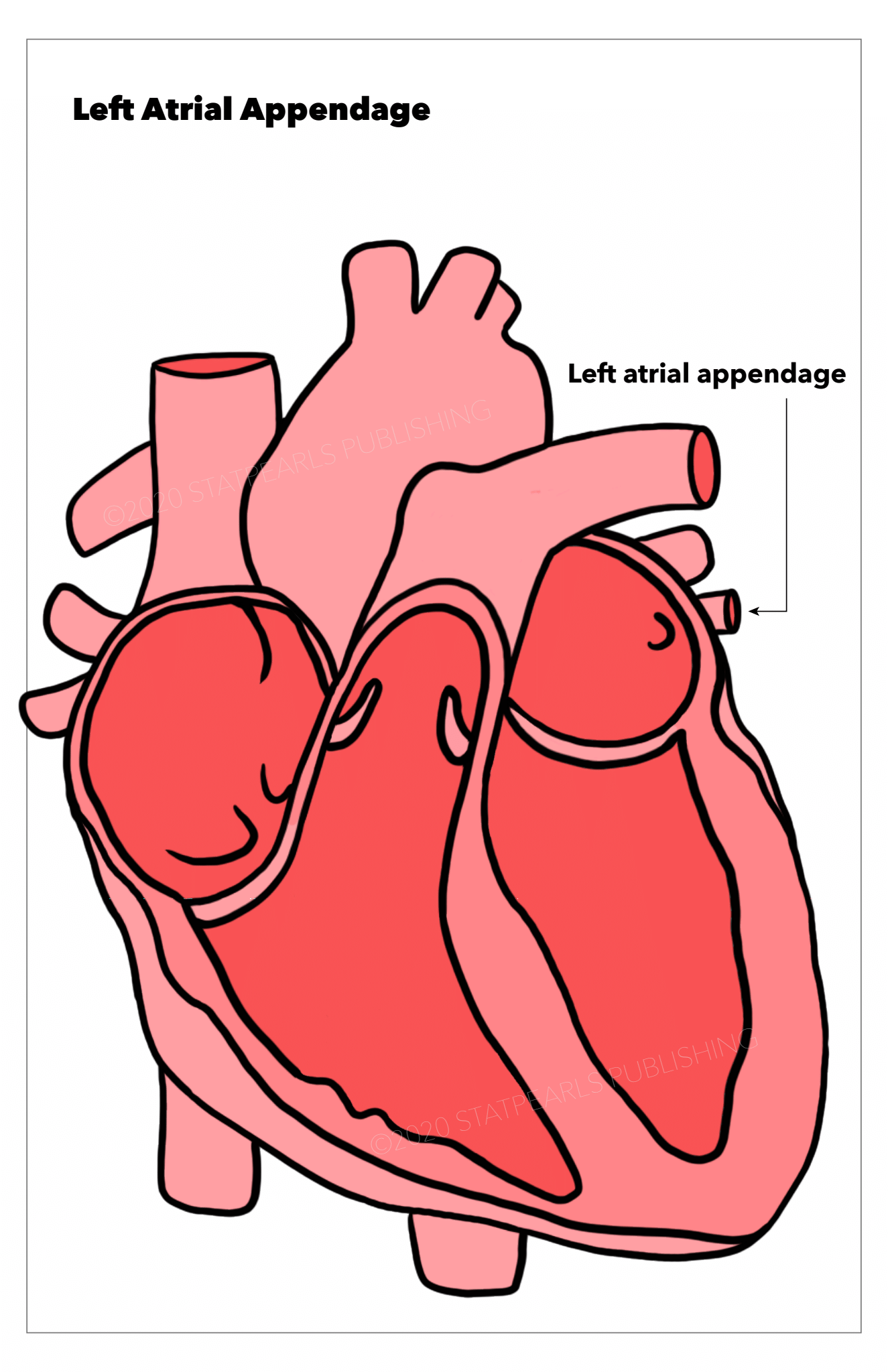
Left atrial appendage, heart Illustration by Emma Gregory
(Click Image to Enlarge)
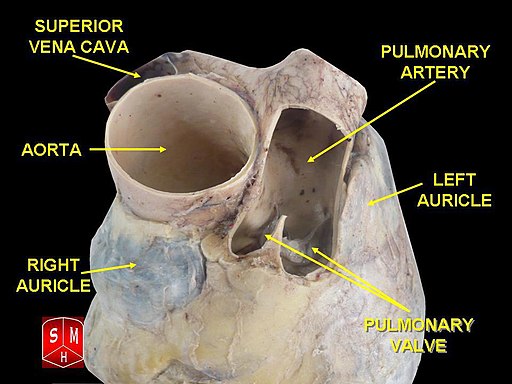
Cadaveric dissection of human heart showing left atrial appendage (left auricle)
Anatomist90, CC BY-SA 3.0 , via Wikimedia Commons
(Click Image to Enlarge)
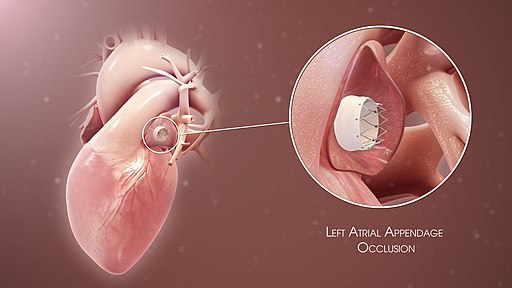
Illustration of left atrial appendage occlusion device used for stroke prevention in patients with atrial fibrillation
Scientific Animations, CC BY-SA 4.0 , via Wikimedia Commons
(Click Image to Enlarge)
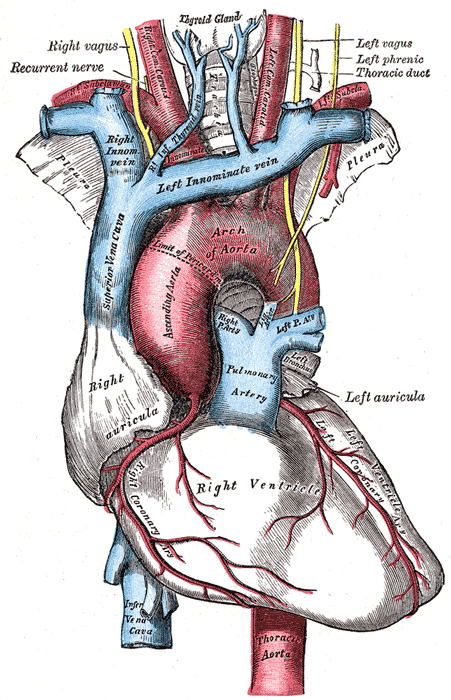
Anatomy drawing of heart and related structures
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
References
Al-Saady NM, Obel OA, Camm AJ. Left atrial appendage: structure, function, and role in thromboembolism. Heart (British Cardiac Society). 1999 Nov:82(5):547-54 [PubMed PMID: 10525506]
Di Biase L, Natale A, Romero J. Thrombogenic and Arrhythmogenic Roles of the Left Atrial Appendage in Atrial Fibrillation. Circulation. 2018 Oct 30:138(18):2036-2050. doi: 10.1161/CIRCULATIONAHA.118.034187. Epub [PubMed PMID: 30372144]
Di Biase L, Santangeli P, Anselmino M, Mohanty P, Salvetti I, Gili S, Horton R, Sanchez JE, Bai R, Mohanty S, Pump A, Cereceda Brantes M, Gallinghouse GJ, Burkhardt JD, Cesarani F, Scaglione M, Natale A, Gaita F. Does the left atrial appendage morphology correlate with the risk of stroke in patients with atrial fibrillation? Results from a multicenter study. Journal of the American College of Cardiology. 2012 Aug 7:60(6):531-8. doi: 10.1016/j.jacc.2012.04.032. Epub [PubMed PMID: 22858289]
Level 2 (mid-level) evidenceWang Y, Di Biase L, Horton RP, Nguyen T, Morhanty P, Natale A. Left atrial appendage studied by computed tomography to help planning for appendage closure device placement. Journal of cardiovascular electrophysiology. 2010 Sep:21(9):973-82. doi: 10.1111/j.1540-8167.2010.01814.x. Epub [PubMed PMID: 20550614]
Beigel R, Wunderlich NC, Ho SY, Arsanjani R, Siegel RJ. The left atrial appendage: anatomy, function, and noninvasive evaluation. JACC. Cardiovascular imaging. 2014 Dec:7(12):1251-65. doi: 10.1016/j.jcmg.2014.08.009. Epub [PubMed PMID: 25496544]
Level 3 (low-level) evidenceMajunke N, Sandri M, Adams V, Daehnert I, Mangner N, Schuler G, Moebius-Winkler S. Atrial and Brain Natriuretic Peptide Secretion After Percutaneous Closure of the Left Atrial Appendage With the Watchman Device. The Journal of invasive cardiology. 2015 Oct:27(10):448-52 [PubMed PMID: 25999139]
Baxter GF. The natriuretic peptides. Basic research in cardiology. 2004 Mar:99(2):71-5 [PubMed PMID: 14963664]
Level 3 (low-level) evidenceCurry FR. Atrial natriuretic peptide: an essential physiological regulator of transvascular fluid, protein transport, and plasma volume. The Journal of clinical investigation. 2005 Jun:115(6):1458-61 [PubMed PMID: 15931381]
Level 3 (low-level) evidencePotter LR, Yoder AR, Flora DR, Antos LK, Dickey DM. Natriuretic peptides: their structures, receptors, physiologic functions and therapeutic applications. Handbook of experimental pharmacology. 2009:(191):341-66. doi: 10.1007/978-3-540-68964-5_15. Epub [PubMed PMID: 19089336]
Level 3 (low-level) evidenceMukoyama M, Nakao K, Hosoda K, Suga S, Saito Y, Ogawa Y, Shirakami G, Jougasaki M, Obata K, Yasue H. Brain natriuretic peptide as a novel cardiac hormone in humans. Evidence for an exquisite dual natriuretic peptide system, atrial natriuretic peptide and brain natriuretic peptide. The Journal of clinical investigation. 1991 Apr:87(4):1402-12 [PubMed PMID: 1849149]
Sherif HM. The developing pulmonary veins and left atrium: implications for ablation strategy for atrial fibrillation. European journal of cardio-thoracic surgery : official journal of the European Association for Cardio-thoracic Surgery. 2013 Nov:44(5):792-9. doi: 10.1093/ejcts/ezt098. Epub 2013 Feb 27 [PubMed PMID: 23447471]
Regazzoli D, Ancona F, Trevisi N, Guarracini F, Radinovic A, Oppizzi M, Agricola E, Marzi A, Sora NC, Della Bella P, Mazzone P. Left Atrial Appendage: Physiology, Pathology, and Role as a Therapeutic Target. BioMed research international. 2015:2015():205013. doi: 10.1155/2015/205013. Epub 2015 Jul 7 [PubMed PMID: 26236716]
AlTurki A, Huynh T, Dawas A, AlTurki H, Joza J, Healey JS, Essebag V. Left atrial appendage isolation in atrial fibrillation catheter ablation: A meta-analysis. Journal of arrhythmia. 2018 Oct:34(5):478-484. doi: 10.1002/joa3.12095. Epub 2018 Jul 20 [PubMed PMID: 30327692]
Level 1 (high-level) evidenceWhitlock RP, Belley-Cote EP, Paparella D, Healey JS, Brady K, Sharma M, Reents W, Budera P, Baddour AJ, Fila P, Devereaux PJ, Bogachev-Prokophiev A, Boening A, Teoh KHT, Tagarakis GI, Slaughter MS, Royse AG, McGuinness S, Alings M, Punjabi PP, Mazer CD, Folkeringa RJ, Colli A, Avezum Á, Nakamya J, Balasubramanian K, Vincent J, Voisine P, Lamy A, Yusuf S, Connolly SJ, LAAOS III Investigators. Left Atrial Appendage Occlusion during Cardiac Surgery to Prevent Stroke. The New England journal of medicine. 2021 Jun 3:384(22):2081-2091. doi: 10.1056/NEJMoa2101897. Epub 2021 May 15 [PubMed PMID: 33999547]
Lip GY, Nieuwlaat R, Pisters R, Lane DA, Crijns HJ. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the euro heart survey on atrial fibrillation. Chest. 2010 Feb:137(2):263-72. doi: 10.1378/chest.09-1584. Epub 2009 Sep 17 [PubMed PMID: 19762550]
Level 2 (mid-level) evidencePage RL. The Closing Argument for Surgical Left Atrial Appendage Occlusion. The New England journal of medicine. 2021 Jun 3:384(22):2154-2155. doi: 10.1056/NEJMe2106069. Epub 2021 May 15 [PubMed PMID: 33999543]
Mahmood E, Matyal R, Mahmood F, Xu X, Sharkey A, Chaudhary O, Karani S, Khabbaz K. Impact of Left Atrial Appendage Exclusion on Short-Term Outcomes in Isolated Coronary Artery Bypass Graft Surgery. Circulation. 2020 Jul 7:142(1):20-28. doi: 10.1161/CIRCULATIONAHA.119.044642. Epub 2020 Jun 3 [PubMed PMID: 32489114]
Holmes DR, Reddy VY, Turi ZG, Doshi SK, Sievert H, Buchbinder M, Mullin CM, Sick P, PROTECT AF Investigators. Percutaneous closure of the left atrial appendage versus warfarin therapy for prevention of stroke in patients with atrial fibrillation: a randomised non-inferiority trial. Lancet (London, England). 2009 Aug 15:374(9689):534-42. doi: 10.1016/S0140-6736(09)61343-X. Epub [PubMed PMID: 19683639]
Level 1 (high-level) evidenceHolmes DR Jr, Kar S, Price MJ, Whisenant B, Sievert H, Doshi SK, Huber K, Reddy VY. Prospective randomized evaluation of the Watchman Left Atrial Appendage Closure device in patients with atrial fibrillation versus long-term warfarin therapy: the PREVAIL trial. Journal of the American College of Cardiology. 2014 Jul 8:64(1):1-12. doi: 10.1016/j.jacc.2014.04.029. Epub [PubMed PMID: 24998121]
Level 1 (high-level) evidenceLópez-López JA, Sterne JAC, Thom HHZ, Higgins JPT, Hingorani AD, Okoli GN, Davies PA, Bodalia PN, Bryden PA, Welton NJ, Hollingworth W, Caldwell DM, Savović J, Dias S, Salisbury C, Eaton D, Stephens-Boal A, Sofat R. Oral anticoagulants for prevention of stroke in atrial fibrillation: systematic review, network meta-analysis, and cost effectiveness analysis. BMJ (Clinical research ed.). 2017 Nov 28:359():j5058. doi: 10.1136/bmj.j5058. Epub 2017 Nov 28 [PubMed PMID: 29183961]
Level 1 (high-level) evidencePerrotta L, Bordignon S, Dugo D, Fürnkranz A, Konstantinou A, Ricciardi G, Pieragnoli P, Schmidt B, Chun KJ. Complications From Left Atrial Appendage Exclusion Devices. Journal of atrial fibrillation. 2014 Jun-Jul:7(1):1034. doi: 10.4022/jafib.1034. Epub 2014 Jun 30 [PubMed PMID: 27957078]
Sakellaridis T, Argiriou M, Charitos C, Tsakiridis K, Zarogoulidis P, Katsikogiannis N, Kougioumtzi I, Machairiotis N, Tsiouda T, Arikas S, Mpakas A, Beleveslis T, Koletas A, Zarogoulidis K. Left atrial appendage exclusion-Where do we stand? Journal of thoracic disease. 2014 Mar:6 Suppl 1(Suppl 1):S70-7. doi: 10.3978/j.issn.2072-1439.2013.10.24. Epub [PubMed PMID: 24672702]
Lakkireddy D, Turagam M, Afzal MR, Rajasingh J, Atkins D, Dawn B, Di Biase L, Bartus K, Kar S, Natale A, Holmes DJ Jr. Left Atrial Appendage Closure and Systemic Homeostasis: The LAA HOMEOSTASIS Study. Journal of the American College of Cardiology. 2018 Jan 16:71(2):135-144. doi: 10.1016/j.jacc.2017.10.092. Epub [PubMed PMID: 29325636]
Yaghi S, Song C, Gray WA, Furie KL, Elkind MS, Kamel H. Left Atrial Appendage Function and Stroke Risk. Stroke. 2015 Dec:46(12):3554-9. doi: 10.1161/STROKEAHA.115.011273. Epub 2015 Oct 27 [PubMed PMID: 26508750]
Salooja MS, Singla M, Srivastava A, Mukherjee KC. Isolated tear in left atrial appendage due to blunt trauma chest: A rare case report. Journal of the Saudi Heart Association. 2013 Apr:25(2):95-7. doi: 10.1016/j.jsha.2012.11.001. Epub 2012 Nov 24 [PubMed PMID: 24174854]
Level 3 (low-level) evidenceScorpio RJ, Wesson DE, Smith CR, Hu X, Spence LJ. Blunt cardiac injuries in children: a postmortem study. The Journal of trauma. 1996 Aug:41(2):306-9 [PubMed PMID: 8760541]