Introduction
To maintain a stable perception of the world around us while we engage in normal movements throughout our day, such as walking, we have something known as the vestibulo-ocular reflex (VOR). This reflex keeps us steady and balanced even though our eyes and head are continuously moving when we perform most actions. When we make a head movement, our eye muscles are triggered instantly to create an eye movement opposite to that of our head movement at the exact same speed to readjust the visual world, which, in turn, stabilizes our retinal image by keeping the eye still in space and focused on an object, despite the head motion.[1]
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The vestibulo-ocular reflex involves three parts[1]:
- A peripheral sensory apparatus (which consists of a set of motion sensors: the semicircular canals and the otolith organs (saccule and utricle)
- A central processing mechanism
- A motor output (which are the eye muscles)
Otolith organs are sensitive to linear acceleration and therefore detect the position of the head relative to gravity and head translation. Semicircular canals, however, are responsible for detecting head rotation since these are sensitive to angular acceleration. These organize in a push-pull structure consisting of one coplanar canal on the left side and another coplanar canal on the right side, which work by coordinating with each other. Humans have a total of six canals arranged in three main planes (anterior, posterior, horizontal) on both sides; each plane has a pair of canals. A canal will get stimulated by head motion towards that canal.[2] When a canal on one side is activated, there is inhibition of the other one during angular head movements. When there are head movements and rotation, the velocity of the movements dictates the difference in firing rate between the two semicircular canals. Hair cells are embedded in a fluid and gelatinous structure called the ampulla in each canal. When our heads rotate, the canal will move relative to the fluid inside of it, which will create a force against the ampulla, causing hair cells to bend. When the head is at rest, vestibular afferents have tonic discharge; this results in a balance between the semicircular canal pairs. Cases of nystagmus and ocular misalignment may be interpreted by understanding the organization and structure of the semicircular canals and otolith organs within the head.[1] Information regarding linear acceleration, angular velocity, and orientation of the head relative to gravity are all collected by these peripheral motion sensors. These sensors relay this information to the central nervous system. Here, information from somatosensors (carrying other sensory information) is combined with motion sensory information to calculate head orientation.
The central nervous system (CNS) is the central processing mechanism, which sends its outputs to the spinal cord and ocular muscles to generate the VOR. Each SSC has excitatory projections to a pair of extraocular muscles in each eye and inhibitory projections to an antagonistic pair of muscles.[2] In addition to the VOR, we also have a vestibulospinal reflex (VSR), which prevents falls by maintaining head and postural stability. It does this by creating compensatory body movements.[1] To attain an even better orientation, this information also goes to cortical structures (posterior insular vestibular cortex (PIVC)) for further integration with tactile, auditory, and proprioceptive inputs. Actions of the VOR and VSR becomes controlled and continuously adjusted as needed by the CNS.[1]
Embryology
Research done on mice and rats shows that vestibular afferents and central neurons have some functionality very early in life. This research suggests that neural network connections between vestibular afferents, central neurons, oculomotor neurons, and extraocular eye muscles are initiated and set up to some extent by birth. Much of this maturation process was shown to be dependent on the growth of the animal and its vestibular organs. Although the development and maturation of the VOR did not seem to be influenced by the presence or absence of visual inputs initially, this was noted to be crucial for the fine-tuning and enhancement of the VOR.[3] The reflex becomes impaired in individuals who are blind.[4]
Blood Supply and Lymphatics
The primary blood supply for the peripheral vestibular system is the labyrinthine artery, which comes from the anterior inferior cerebellar artery. The utricle, small part of the saccule, and superior and horizontal semicircular canals receive supply by the superior vestibular artery, which bifurcates with the anterior inferior cerebellar artery. The cochlea, rest of the saccule, and most of the posterior semicircular canal get supplied by bifurcation of the common cochlear artery. The superior vein drains the horizontal and superior semicircular canal and utricle. The inferior vein is responsible for draining the posterior semicircular canals and saccule.[5]
Nerves
Vestibular information comes into the brainstem via the cranial nerve VIII. Signals enter the vestibular nuclear complex, located in the medulla and pons. Four main nuclei comprise the vestibular nuclear complex (superior, inferior, medial, and lateral).[6] Using first-order sensory neurons of cranial nerve V, most of the semicircular canal inputs synapse at the superior and medial nuclei. The medial longitudinal fasciculus is used to send second-order sensory neuron signals ipsi- and contra-laterally to oculomotor cranial nerves III, IV, and VI. Lastly, a third motor neuron is responsible for stimulating the extraocular muscles that cause conjugate eye movements.[7] Also, the vestibular system sends information via the inferior cerebellar peduncle to the cerebellum to modulate the VOR. The flocculonodular lobe and fastigial nuclei are responsible for this fine-tuning. Vestibular data is also processed by the cerebellum, which then aids in the regulation of vestibular reflexes, maintaining posture, and coordination.[5] Other connections to the cerebral cortex, thalamus, and reticular formation assist in coordinating efforts between other central networks and the vestibular system, allowing for enhanced spatial awareness.[7]
Muscles
As mentioned earlier, the VOR works by activating our eye muscles to create eye movements in the exact speed but opposite direction of our head movements to stabilize our retinal images.[1] To recognize the effects of this activation, we must understand the direction of pull on the various eye muscles at play. The horizontal recti are easier to understand than the vertical recti and obliques, which are more complex. The lateral rectus is responsible for abducting the eye, while the medial rectus is responsible for adducting the eye (horizontal recti). The effect of pull on the vertical recti and oblique muscles changes depending on whether the eye is abducted or adducted. When the eye is in abduction, the contraction of the superior rectus will elevate the eye and contraction of the inferior rectus will depress the eye. When the eye moves into adduction, there is more of an intorsional movement caused by the superior rectus and an extorsional movement caused by contraction of the inferior rectus.[8] During eye abduction, contraction of superior oblique causes intorsion of the eye and contraction of inferior oblique causes extorsion., whereas during adduction, contraction of superior oblique causes depression and contraction of inferior oblique causes elevation.[8]
Surgical Considerations
Surgery is not the first-line of treatment for VOR malfunction. The ability to restore the VOR function varies. Due to neuroplasticity, it usually improves spontaneously with time, and no intervention is needed. There are a few suggested interventions for those who do not recover with time. One is an adaptation, and another is exercise-based treatment programs (vestibular rehabilitation therapy). However, it is challenging to restore the VOR function at high velocities in severe cases of vestibular loss.[9] The goal of vestibular rehabilitation therapy (VRT) is to practice head and eye movements with different activities and postures. They should repeat movements that stimulate vertigo and continue to expose patients to different types of sensory and motor environments.[10] VOR exercises should start with patients in a seated, still position to assess if there is an aggravation of symptoms such as dizziness, nausea, and anxiety. The exercises can slowly increase in velocity. By gradually increasing the intensity, the capacity of the VOR system will not be overwhelmed. Other methods to rehabilitate the VOR function are under development. For example, researchers found that artificial restoration of the VOR function is possible by electrically stimulating the LAN branch of the vestibular branch in humans.[11]
Clinical Significance
The implications of a disrupted vestibulo-ocular reflex include oscillopsia and abnormal nystagmus.[12] Oscillopsia results in blurred vision when the head is in motion and objects appear to jiggle and bounce since they do not stay fixed at one point in the retina.[13] Patients are often forced to stop and stay still to read signs. Reading a book may also require great effort since small head movements may cause distortion. Since these patients would need more time to comprehend and process words and letters, undiagnosed children are sometimes wrongly thought to have dyslexia or dyscalculia. Abnormal nystagmus may also blur vision since it causes excessive involuntary eye movements (can be in various directions; side to side or up and down).[14][15] Individuals with VOR malfunction are also likely to be clumsy, get motion sick easily, have sensory issues, difficulty maintaining balance, and nausea. If the sensory vestibular organs are not fully functional on either side, the brain will receive conflicting signals regarding movement, causing vertigo.[16][17][18]
Other Issues
Assessment of the vestibulo-ocular reflex takes place using the Halmagyi-Curthoys test, also known as the rapid impulse test. To perform this, the physician will rapidly move the patient’s head in one direction (left or right), and the eyes should remain in place focused on a particular object in front of them despite the head movement. If a patient’s VOR has damage on one side when their head turns to that direction with force, their eyes will follow the direction of the head movement before coming back to their focal point; this would imply some issue in the vestibulo-ocular reflex arc.[19] The VOR may also be tested using the caloric reflex test, where cold water or warm water is poured into the patient’s external auditory canal using a syringe to induce nystagmus. When using cold water, the fast phase of nystagmus should be to the opposite side of the ear filled with the water. However, when using warm water, the fast phase of nystagmus should be on the same side as the water-filled ear. If this eye movement is abnormal and not occurring as described in the patient, there is likely vestibular dysfunction in the side being stimulated by water.[20] Brain death is a complete loss of cerebral function.[21] If performing the caloric reflex test and the VOR is absent in the patient, this is likely a serious indicator of brain death.[22]
Media
(Click Image to Enlarge)
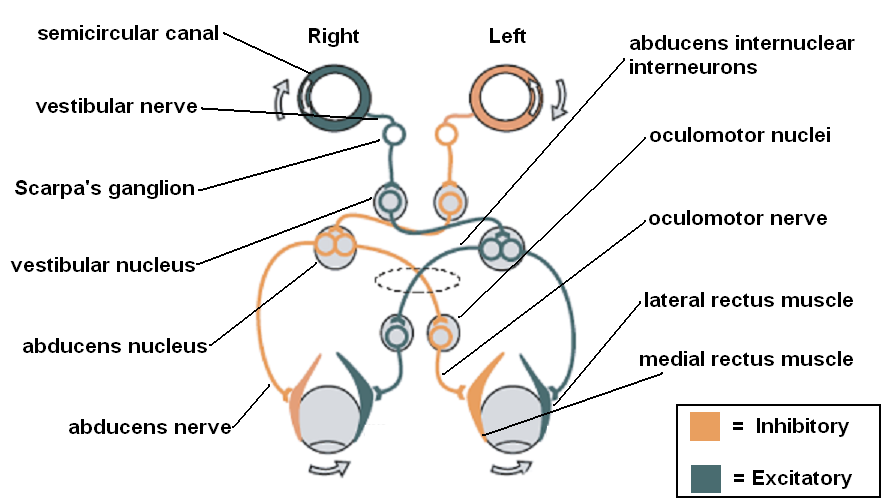
Vestibulo-ocular reflex Courtesy: https://commons.wikimedia.org/wiki/File:Vestibulo-ocular_reflex.PNG
References
Fetter M. Vestibulo-ocular reflex. Developments in ophthalmology. 2007:40():35-51 [PubMed PMID: 17314478]
Level 3 (low-level) evidenceSherman KR, Keller EL. Vestibulo-ocular reflexes of adventitiously and congenitally blind adults. Investigative ophthalmology & visual science. 1986 Jul:27(7):1154-9 [PubMed PMID: 3487529]
Lisberger SG, Pavelko TA, Broussard DM. Responses during eye movements of brain stem neurons that receive monosynaptic inhibition from the flocculus and ventral paraflocculus in monkeys. Journal of neurophysiology. 1994 Aug:72(2):909-27 [PubMed PMID: 7983546]
Level 3 (low-level) evidenceBronstein AM, Patel M, Arshad Q. A brief review of the clinical anatomy of the vestibular-ocular connections-how much do we know? Eye (London, England). 2015 Feb:29(2):163-70. doi: 10.1038/eye.2014.262. Epub 2014 Nov 21 [PubMed PMID: 25412719]
Carleton SC, Carpenter MB. Afferent and efferent connections of the medial, inferior and lateral vestibular nuclei in the cat and monkey. Brain research. 1983 Nov 14:278(1-2):29-51 [PubMed PMID: 6315158]
Level 3 (low-level) evidenceBrandt T, Dieterich M. Vestibular syndromes in the roll plane: topographic diagnosis from brainstem to cortex. Annals of neurology. 1994 Sep:36(3):337-47 [PubMed PMID: 8080241]
Wallace B, Lifshitz J. Traumatic brain injury and vestibulo-ocular function: current challenges and future prospects. Eye and brain. 2016:8():153-164. doi: 10.2147/EB.S82670. Epub 2016 Sep 6 [PubMed PMID: 28539811]
Spencer RF, Porter JD. Biological organization of the extraocular muscles. Progress in brain research. 2006:151():43-80 [PubMed PMID: 16221585]
Level 3 (low-level) evidenceCurthoys IS, Halmagyi GM. Vestibular compensation: a review of the oculomotor, neural, and clinical consequences of unilateral vestibular loss. Journal of vestibular research : equilibrium & orientation. 1995 Mar-Apr:5(2):67-107 [PubMed PMID: 7743004]
Level 3 (low-level) evidenceHan BI, Song HS, Kim JS. Vestibular rehabilitation therapy: review of indications, mechanisms, and key exercises. Journal of clinical neurology (Seoul, Korea). 2011 Dec:7(4):184-96. doi: 10.3988/jcn.2011.7.4.184. Epub 2011 Dec 29 [PubMed PMID: 22259614]
Perez Fornos A, Guinand N, van de Berg R, Stokroos R, Micera S, Kingma H, Pelizzone M, Guyot JP. Artificial balance: restoration of the vestibulo-ocular reflex in humans with a prototype vestibular neuroprosthesis. Frontiers in neurology. 2014:5():66. doi: 10.3389/fneur.2014.00066. Epub 2014 Apr 29 [PubMed PMID: 24808890]
Fife TD, Tusa RJ, Furman JM, Zee DS, Frohman E, Baloh RW, Hain T, Goebel J, Demer J, Eviatar L. Assessment: vestibular testing techniques in adults and children: report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology. 2000 Nov 28:55(10):1431-41 [PubMed PMID: 11094095]
Eckhardt-Henn A, Breuer P, Thomalske C, Hoffmann SO, Hopf HC. Anxiety disorders and other psychiatric subgroups in patients complaining of dizziness. Journal of anxiety disorders. 2003:17(4):369-88 [PubMed PMID: 12826087]
Cha YH, Lee H, Santell LS, Baloh RW. Association of benign recurrent vertigo and migraine in 208 patients. Cephalalgia : an international journal of headache. 2009 May:29(5):550-5. doi: 10.1111/j.1468-2982.2008.01770.x. Epub 2009 Jan 16 [PubMed PMID: 19170697]
Takahashi M, Okada Y, Saito A, Takei Y, Tomizawa I, Uyama K, Takeuti I, Kanzaki J. Roles of head, gaze, and spatial orientation in the production of oscillopsia. Journal of vestibular research : equilibrium & orientation. 1990-1991:1(3):215-22 [PubMed PMID: 1670155]
Kaminski HJ, Leigh RJ. International Symposium for Therapy of Ocular Motility and Related Visual Disturbances. Neurology. 1997 May:48(5):1178-84 [PubMed PMID: 9153439]
Guinand N, Pijnenburg M, Janssen M, Kingma H. Visual acuity while walking and oscillopsia severity in healthy subjects and patients with unilateral and bilateral vestibular function loss. Archives of otolaryngology--head & neck surgery. 2012 Mar:138(3):301-6. doi: 10.1001/archoto.2012.4. Epub [PubMed PMID: 22431876]
Level 2 (mid-level) evidenceLambert S, Sigrist A, Delaspre O, Pelizzone M, Guyot JP. Measurement of dynamic visual acuity in patients with vestibular areflexia. Acta oto-laryngologica. 2010 Jul:130(7):820-3. doi: 10.3109/00016480903426592. Epub [PubMed PMID: 20082568]
Level 2 (mid-level) evidenceMcGarvie LA, MacDougall HG, Halmagyi GM, Burgess AM, Weber KP, Curthoys IS. The Video Head Impulse Test (vHIT) of Semicircular Canal Function - Age-Dependent Normative Values of VOR Gain in Healthy Subjects. Frontiers in neurology. 2015:6():154. doi: 10.3389/fneur.2015.00154. Epub 2015 Jul 8 [PubMed PMID: 26217301]
Gonçalves DU, Felipe L, Lima TM. Interpretation and use of caloric testing. Brazilian journal of otorhinolaryngology. 2008 May-Jun:74(3):440-6 [PubMed PMID: 18661020]
Level 1 (high-level) evidenceWijdicks EF. Determining Brain Death. Continuum (Minneapolis, Minn.). 2015 Oct:21(5 Neurocritical Care):1411-24. doi: 10.1212/CON.0000000000000221. Epub [PubMed PMID: 26426238]
Meneses E, Sampaio A, Venosa A, Tauil P, Dias M, Oliveira C. Vestibulo-ocular reflex as predictor of cerebral death in comatose patients. The international tinnitus journal. 2010:16(1):8-13 [PubMed PMID: 21609907]