Introduction
The cerebellum, meaning "little brain" in Latin, is primarily responsible for the coordination of movement, maintaining posture and balance, muscle tone, and motor learning. Recent research has shown that the cerebellum may also have cognitive functions, but the exact mechanism and pathways are still unclear. In this chapter, we present the gross and functional anatomy of the cerebellum and then focus on the structures that are involved in clinical presentations and syndromes.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
Gross Anatomy
The cerebellum is in the posterior cranial fossa posterior to the brainstem and the fourth ventricle. It is covered by the tentorium cerebelli anteriorly and superiorly. When looking at the cerebellum from behind, it has two hemispheres which are joined together by a longitudinal depression running down the midline of both hemispheres called the vermis. The cerebellar cortical surface is convoluted into numerous folia. The midsagittal view of these folia resembles a branching tree, called the arbor vitae, meaning tree of life in Latin.[1]
When looking at the cerebellum from the side, it's divided into three anatomical lobes, anterior, posterior and flocculonodular lobes, separated by two fissures, the primary and posterolateral fissures. The anterior and posterior lobes are separated from each other by the primary fissure, and the posterolateral fissure separates the posterior and flocculonodular lobe. The flocculonodular lobe lies on the inferior surface of the cerebellum. The cerebellar tonsils are round lobes situated on the undersurface of the cerebellar hemispheres, just inferior to the flocculonodular lobe.[1]
There are four pairs of gray matter nuclei (or deep cerebellar nuclei) in the cerebellum. Starting from the most lateral to the most medial nuclei, they are called dentate, emboliform, globose and fastigial nuclei. Together, the emboliform and globose nuclei have the collective name of the nuclei interpositum.[2] The deep cerebellar nuclei are the primary source of information output from the cerebellum. One exception to this is that the flocculonodular lobe synapses with the vestibular nuclei and these synapses do not pass through the deep cerebellar nuclei before leaving the cerebellum.
Functionally, the cerebellum divides into three zones, the vestibulocerebellum, cerebrocerebellum, and spinocerebellum (Figure 1).[1]
Vestibulocerebellum
The flocculonodular lobe, also called the vestibulocerebellum, mainly receives input from the ipsilateral vestibular nuclei. It receives additional input from the pretectal area of the midbrain and the visual cortex. Efferents from the flocculonodular lobe relay signals directly to the vestibular nuclei, bypassing the deep cerebellar nuclei. This area is primarily responsible for balance and ocular movements. While the medial part of the flocculonodular lobe (the nodulus) helps maintain balance, the flocculus mediates the vestibulo-ocular adaptation contributing to the smooth pursuit eye movements such as following a slow-moving object with one's eyes. The vestibulo-ocular reflex, a reflex that functions to stabilize the image on the retina during head movement by causing the eyes to move in the opposite direction of the head, is also part of the vestibulo-ocular adaptation.[3]
Spinocerebellum
The spinocerebellum is made up of the vermis (a longitudinal depression in the medial part of the cerebellar hemispheres) and paravermis (intermediate portions of the cerebellar hemispheres; just lateral to the vermis). The spinocerebellum receives somatosensory input from both the ipsilateral face (through the trigeminal nucleus) and body (through the dorsal column of the spinal cord). The primary function of the spinocerebellum is coordination of motor movements and maintenance of muscular tone.
The vermis area coordinates the movements of the central body (e.g., trunk, head, proximal limbs) and the paravermis area coordinates movement from the distal limbs (e.g., arms, legs, fingers, toes).
The dorsal vermis connects to the fastigial nuclei, both of which modulate saccadic eye movements, (eye movements that rapidly move both eyes from one object to another) and vergence eye movements (moving both eyes away from each other to focus on an image in the distance; opposite of divergence).[4]
The spinocerebellum has connections to the rubrospinal tract thus modulating muscular tone in the flexor muscles of the body as well as connections to the vestibulospinal tract thus modulating muscular tone in the extensor muscles of the body as well.
Cerebrocerebellum
The cerebellar hemispheres (excluding the vermis and paravermis) are called the cerebrocerebellum. The cerebellar hemispheres function in motor planning, the timing of the onset of movements, and their coordination. Cerebrocerebellum mainly receives input from the primary cerebral motor cortex and the supplementary motor areas via the contralateral corticopontocerebellar fibers. It receives additional input from the contralateral inferior olivary nucleus.
The Purkinje cells send outputs to the dentate and interposed nuclei which project fibers to the contralateral red nucleus (via the cerebellorubral fibers) and ventrolateral thalamic nuclei (via the cerebellothalamic fibers). The ventrolateral thalamic nucleus then relays the signals to the cerebral premotor, and motor cortex and the red nucleus relays the signals to the olivary nuclei.
The cerebellum is connected to the brainstem by the superior, middle, and inferior peduncles. The largest of the three is the middle peduncle, which contains the pontocerebellar tract. This tract provides afferent information from the contralateral pontine nuclei, which obtain their input from the primary motor cortex and supplementary motor areas. The inferior cerebellar peduncle contains afferent fibers, including dorsal spinocerebellar tract, cuneocerebellar tract, olivocerebellar tract, and vestibulocerebellar tract. The superior cerebellar peduncle conveys efferent information from the deep cerebellar nuclei to the motor nuclei of the thalamus and the red nucleus.
Microstructure
Three layers comprise the cerebellar cortex as opposed to the six layers of the cerebral cortex. These are the granular layer, Purkinje cell layer, and the molecular layer. Purkinje cells provide inhibitory signals to the deep cerebellar nuclei, whereas the deep cerebellar nuclei provide excitatory signals to the efferent nerve fiber tracts.[5]
Embryology
During the 3rd week of embryogenesis, the blastocyst is reorganized into a 3 layer structure, a process known as gastrulation. The layers are the endoderm, mesoderm, and ectoderm. The notochord (a transient embryonic structure just below the ectoderm which later becomes the nucleus pulposus of the intervertebral disk in adults) induces the overlying ectoderm to differentiate into the neural plate. The neural plate then gives rise to the neural tube and neural crest cells. The neural tube gives rise to 3 vesicles, the prosencephalon, mesencephalon, and telencephalon, which will ultimately develop into the brain. The prosencephalon gives rise to the telencephalon (which develops into the cerebral hemispheres and lateral ventricles) and the diencephalon (which develops into the thalamus, hypothalamus, and the third ventricle). The mesencephalon develops into the midbrain and aqueduct of Sylvius. The telencephalon gives rise to the metencephalon (which develops into the pons, cerebellum and the upper part of the fourth ventricle) and the myelencephalon (which develops into the medulla and lower part of the fourth ventricle). It seems that the cerebellar hemispheres develop independently from the cerebellar vermis. At weeks 7-9, the rhombic lip (the posterior part of the developing metencephalon) fuses with the midbrain and the developing choroid plexus to form the cerebellar hemispheres. The cerebellar vermis develops after the cerebellar hemispheres from a cluster of cells near the cerebral aqueduct. The developing cerebellar hemispheres undergo mechanical stress (eg. rotation, shear stress) that lead to the development of fissures found on the surface of the mature cerebellar hemispheres. [6]
Blood Supply and Lymphatics
The cerebellum receives its blood supply from 3 arteries that branch out from the posterior circulation of the brain (also called the vertebrobasilar arterial system, which is the collective term for the 2 vertebral arteries and the basilar artery).
- Superior Cerebellar Artery (SCA): branches off from the superior part of the basilar artery and supplies the superior part of the cerebellum
- Anterior Inferior Cerebellar Artery (AICA): branches off from the middle part of the basilar artery and supplies the anterior-inferior segment of the cerebellum.
- Posterior Inferior Cerebellar Arteries (PICA): branches off from the vertebral arteries and supplies the posterior cerebellum and the inferior cerebellar peduncle.[7]
Clinical Significance
Clinical Presentations associated with cerebellar dysfunction:
Ataxia: Lack of normal coordination of movements.[8]
Gait problems: Lesions of the cerebellum typically affect the same side of the body, and patients fall towards the side of the lesion.
Intention Tremor: Low-frequency tremor (below 5Hz) with voluntary movement of the limb. The tremor is exaggerated when the limb approaches the endpoint of its deliberate movement (cerebellar tremor).[9] The tremor is not present at rest (feature of parkinsonian tremor).
Dysdiadochokinesia: The inability to perform fast, alternating movements.
Decomposition of Movement (abnormal coordination): Movement cannot occur smoothly and gets divided into its components.
Dysmetria: Overshooting or undershooting the target. Patients are unable to reach the target at the first attempt and make corrections.
Dysarthria: This is the inability to articulate words properly.
Signs of Cerebellar Vermis and Flocculonodular Lobe Lesions
Gait Ataxia: Abnormal coordination of movements while walking. Patients have wide-based, drunk like unsteady, stumbling gait, which is also called “staggering gait.” The patient will be unable to walk on toes or heels and in tandem; also known as truncal ataxia.
Titubation: Tremor (noodling) of the head or axial body. If severe, the patient can’t sit or stand without help.
Nystagmus: Commonly bilateral, these are involuntary, rapid, repetitive eye movements, which can be horizontal or vertical.
Signs of Cerebellar Hemisphere (Cerebrocerebellum) Lesions
Limb ataxia: Also referred to as appendicular ataxia. This condition presents with lesions of the intermediate and lateral portions of the cerebellar hemisphere. The degree and locations of ataxia depend on the somatotopic projection of the body parts of the involved cerebellar hemisphere. It can present as dysmetria, dysdiadochokinesis, hypotonia or intention tremor in one or both extremities. Patients can also present with dysarthria.
Developmental Abnormalities
Dandy-Walker syndrome is cerebellar hypoplasia and upward rotation of the cerebellar vermis with cystic dilation of the fourth ventricle.[10]
Joubert Syndrome and rhombencephalosynapsis are rare conditions and seen with cerebellar vermis agenesis.
Pontocerebellar hypoplasias are rare, progressive, familial neurodegenerative disorders, which include PCH gene mutations (tRNA splicing endonuclease subunit genes). There are eleven known subgroups.[11] Signs include cerebellar hypoplasia or atrophy, progressive microcephaly, and different degree of cerebral involvement.
Medulloblastoma is a common tumor of childhood and roots from embryological cells (granular cells).[12]
Chiari I malformation: This is the caudal location of the cerebellar tonsils. Most of the time, it is asymptomatic. Patients may present with headaches. In severe form Chiari I malformation may cause syringomyelia.
Media
(Click Image to Enlarge)
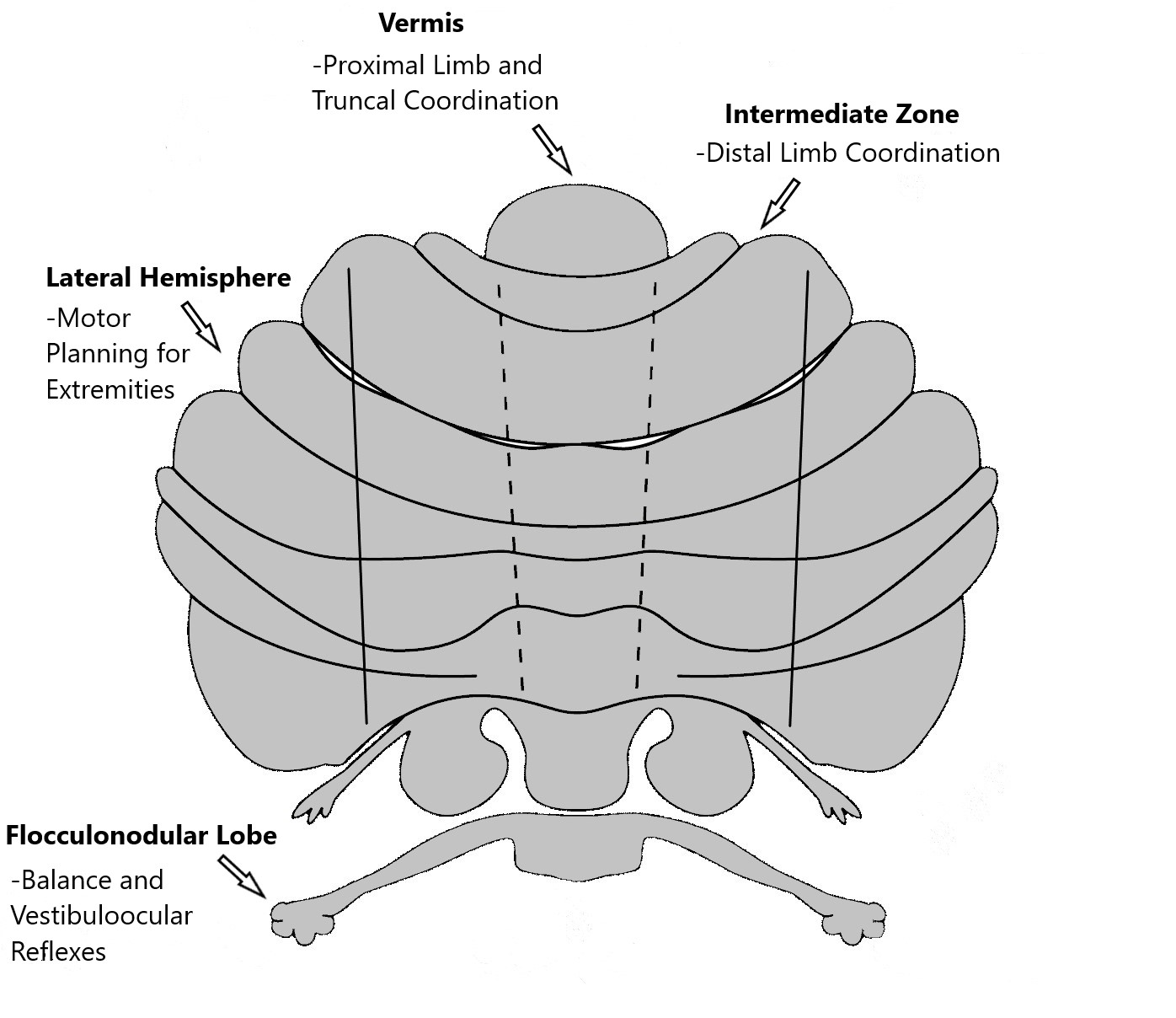
Functional zones of the cerebellum. Contributed by Mahmut Unverdi, MD
References
Roostaei T, Nazeri A, Sahraian MA, Minagar A. The human cerebellum: a review of physiologic neuroanatomy. Neurologic clinics. 2014 Nov:32(4):859-69. doi: 10.1016/j.ncl.2014.07.013. Epub 2014 Oct 24 [PubMed PMID: 25439284]
Schmahmann JD. The cerebellum and cognition. Neuroscience letters. 2019 Jan 1:688():62-75. doi: 10.1016/j.neulet.2018.07.005. Epub 2018 Jul 8 [PubMed PMID: 29997061]
Level 3 (low-level) evidenceIto M. Cerebellar control of the vestibulo-ocular reflex--around the flocculus hypothesis. Annual review of neuroscience. 1982:5():275-96 [PubMed PMID: 6803651]
Level 3 (low-level) evidenceRobinson FR, Fuchs AF. The role of the cerebellum in voluntary eye movements. Annual review of neuroscience. 2001:24():981-1004 [PubMed PMID: 11520925]
Level 3 (low-level) evidenceVoogd J, Glickstein M. The anatomy of the cerebellum. Trends in neurosciences. 1998 Sep:21(9):370-5 [PubMed PMID: 9735944]
Level 3 (low-level) evidenceCho KH, Rodríguez-Vázquez JF, Kim JH, Abe H, Murakami G, Cho BH. Early fetal development of the human cerebellum. Surgical and radiologic anatomy : SRA. 2011 Aug:33(6):523-30. doi: 10.1007/s00276-011-0796-8. Epub 2011 Mar 6 [PubMed PMID: 21380713]
Savoiardo M, Bracchi M, Passerini A, Visciani A. The vascular territories in the cerebellum and brainstem: CT and MR study. AJNR. American journal of neuroradiology. 1987 Mar-Apr:8(2):199-209 [PubMed PMID: 3105277]
Javalkar V, Khan M, Davis DE. Clinical manifestations of cerebellar disease. Neurologic clinics. 2014 Nov:32(4):871-9. doi: 10.1016/j.ncl.2014.07.012. Epub 2014 Oct 24 [PubMed PMID: 25439285]
Level 3 (low-level) evidencePuschmann A, Wszolek ZK. Diagnosis and treatment of common forms of tremor. Seminars in neurology. 2011 Feb:31(1):65-77. doi: 10.1055/s-0031-1271312. Epub 2011 Feb 14 [PubMed PMID: 21321834]
Butts T, Green MJ, Wingate RJ. Development of the cerebellum: simple steps to make a 'little brain'. Development (Cambridge, England). 2014 Nov:141(21):4031-41. doi: 10.1242/dev.106559. Epub [PubMed PMID: 25336734]
Level 3 (low-level) evidencevan Dijk T, Baas F, Barth PG, Poll-The BT. What's new in pontocerebellar hypoplasia? An update on genes and subtypes. Orphanet journal of rare diseases. 2018 Jun 15:13(1):92. doi: 10.1186/s13023-018-0826-2. Epub 2018 Jun 15 [PubMed PMID: 29903031]
Roussel MF, Hatten ME. Cerebellum development and medulloblastoma. Current topics in developmental biology. 2011:94():235-82. doi: 10.1016/B978-0-12-380916-2.00008-5. Epub [PubMed PMID: 21295689]
Level 3 (low-level) evidence