Introduction
The lungs are the most important respiratory organs (see Image. Relationship Of Thoracic Contents And Thoracic Cage Linings). The bony thorax and pleurae protect this organ pair. The lung apices project superiorly through the supraclavicular fossae and their inferior margins slope from the 6th rib at the midclavicular line to the 8th rib at the midaxillary line and the 10th rib at the scapular line. Each lung is divided into lobes and has the alveolus as the basic gas exchange structural unit. Alveolar tissue comprises the lung parenchyma.
The respiratory airways deliver oxygen to the lungs and tissue carbon dioxide to the environment. The tracheobronchial tree is the branching system of the respiratory airways (see Image. Tracheobronchial Tree, Anterior View). The trachea bifurcates into the right and left main bronchi—one for each lung—at the level of the sternal angle. The shorter and wider right main bronchus runs more vertically than the left.
Each main bronchus divides into lobar bronchi, which supply the lung lobes. Each lobar bronchus gives rise to the segmental bronchi, which supply the bronchopulmonary segments. The bronchopulmonary segments divide into terminal bronchioles, which branch into respiratory bronchioles. Respiratory bronchioles give rise to both alveolar ducts and alveoli. Alveoli may extend from the respiratory bronchioles or alveolar ducts. Alveolar sacs are common spaces between alveolar clusters.
The lungs are supplied by the right and left pulmonary arteries, which originate from the pulmonary trunk at the sternal angle. Pulmonary arteries branch into lobar arteries, then segmental arteries. These arteries carry deoxygenated blood and carbon dioxide to the lungs. The blood-air barrier—the site of gas exchange—is composed of the alveolar epithelium and the interfacing pulmonary capillary endothelium. Pulmonary veins receive oxygenated blood from the bronchopulmonary segments on their way to the hilum before returning to the heart. Distal visceral pleural and bronchial veins also drain into the pulmonary veins but carry deoxygenated blood.
Bronchial arteries supply oxygenated blood to the root of the lungs (bronchi) and visceral pleurae. The bronchial veins drain the proximal capillaries branching out from the bronchial arteries. Lung lymphatic vessels drain into the tracheobronchial lymph nodes.
A pulmonary contusion is a lung parenchymal injury that does not lead to lung or pulmonary vascular lacerations. Blunt chest trauma, shock waves from penetrating chest injuries, and explosions can cause this condition. Pulmonary contusions were first described in 1761 by Morgagni, an Italian anatomist. The term "pulmonary contusion" was coined in the 19th century by French military surgeon Dupuytren.[1][2]
Widespread explosive use during World Wars I and II led to increased recognition of pulmonary contusion due to blast injuries. Many soldiers with blast injuries developed pulmonary bleeding without apparent external injuries.[3]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Any chest trauma, blunt, penetrating, or a combination of both, can cause a pulmonary contusion. Other identified causes include explosions, assaults, falls from great heights, motor vehicle accidents, and sports collisions.[4][5] Severe chest injuries often lead to sternal fractures. However, minor chest trauma in older adults tends to produce lung contusions.[6] Pulmonary contusion is a common complication of rib fractures.[7]
Epidemiology
The true prevalence of pulmonary contusions is unknown, as most studies may have selection bias due to the inclusion of small server case samples. However, pulmonary contusions are the most commonly identified lung injuries (30% to 75%) in blunt chest trauma cases, with a mortality rate of 10 to 25%.[8] Blunt thoracic injuries are the second leading cause of death after head and spinal cord injuries.[9][10] Pulmonary contusion is the second leading injury associated with sternal fractures, accounting for a third of cases.[11][12] Though scapular fractures are rare, more than 90% are associated with severe injuries and pulmonary contusion.[13]
Pathophysiology
The pathophysiology of pulmonary contusion is poorly understood. What is known, however, is that the injury disrupts the blood-air barrier, resulting in leakage of blood and interstitial fluids into the alveolar and interstitial spaces. Fluid in the alveolar space produces alveolar edema and decreases the amount of lung surfactant, resulting in alveolar collapse and atelectasis. Decreased lung compliance, ventilation-perfusion mismatch, and intra-pulmonary shunting result from the tissue damage.[14]
Ventilation of the affected lung is impaired as oxygenated air cannot enter the fluid-filled alveoli during inspiration. Reduced oxygenation leads to reflex vasoconstriction and decreased perfusion, resulting in hypoxemia and hypercapnia.[15][16]
Pulmonary contusion activates the immune system, resulting in tissue macrophage activation and leucocyte migration. The production of cytokines, chemokines, arachidonic acid metabolites, oxygen radicals, and complement in the injury site increases. The coagulation cascade is also activated.[17]
The increased inflammatory response impairs neutrophilic apoptosis and increases alveolar epithelial apoptosis. Severe inflammation may cause Acute Respiratory Distress Syndrome (ARDS). Edema and inflammation may also develop in the contralateral intact chest. Concurrent aspiration of gastric acid can complicate a pulmonary contusion by further injuring the lungs and worsening ARDS.[18]
Pulmonary contusion has three possible mechanisms:[19]
- The spalling effect - occurs when a pressure wave encounters a liquid-gas interface like the alveolar wall, thus disrupting the cells' lipid membranes and increasing membrane permeability.
- The inertial effect - tissues with different densities accelerate or decelerate pressure waves at different rates, stripping lighter alveoli away from denser bronchial tissue.
- The implosion effect - happens when a pressure wave encounters tissues with air bubbles and compresses the gas within the tissues. The rebound force overstretches and tears tissues.
Pulmonary contusions can lead to respiratory failure and death.
Histopathology
Pulmonary hemorrhage may be associated with pulmonary contusion. Alveolar or interstitial fluid accumulation was found in World War II soldiers' lung tissue samples, though this finding was initially attributed to fluid resuscitation. Recent animal models have identified interstitial hemorrhage with edema and inflammatory cell infiltration in patients with lung contusion.[20]
History and Physical
Patients with severe chest injuries may present unresponsive, apneic, and pulseless. After a quick primary survey, resuscitation must be started for these individuals regardless of the cause. Once stable, a secondary survey may be initiated.
Pulmonary contusion presents variably, depending on the severity of the condition. Breathing difficulty, chest pain, and hemoptysis may be elicited in patients with severe pulmonary contusion. Individuals with mild injury may be asymptomatic. A history of trauma typically precedes the symptoms, warranting an investigation for concurrent injuries.
Patients with severe pulmonary contusion are tachypneic, tachycardic, and visibly in respiratory distress in the early stages. Oxygen saturation is low. Chest retractions, jugular distension, and cyanosis may also be observed. Auscultation will reveal decreased breath sounds. Injuries to other parts of the body may also be noted. Cardiorespiratory decompensation may occur in the advanced stages of a pulmonary contusion. Patients may present with hypotension, bradypnea or apnea, altered sensorium, and bradycardia.
In severe contusion, symptoms appear within hours. In mild injury, symptoms may develop gradually over 24 to 48 hours.[21][37]
Evaluation
A detailed history of the injury, thorough physical examination, and imaging can aid in diagnosing pulmonary contusion. The imaging techniques include radiography of the chest, computer tomography (CT) scans, and ultrasound.
The chest x-ray is the most commonly used diagnostic imaging technique (see Image. Pulmonary Contusion Radiograph). However, the image's interpretation may be difficult as lung anatomical boundaries do not limit pulmonary contusions. The presence of a pneumothorax or hemothorax may obscure other injuries. Contusion signs may not appear on chest x-rays immediately after the injury and may be delayed for 6 to 48 hours.[22]
A mild contusion appears as ground-glass haziness on a chest x-ray, while severe disease may mimic pneumonia consolidation.[23] However, pneumonia consolidation is confined to specific areas, while pulmonary contusions can cross fissures. Computed tomography (CT) is recommended if the chest x-ray is equivocal.[24]
A chest CT scan is more sensitive in diagnosing pulmonary contusion than plain films. A higher CT resolution can detect contusion immediately after trauma.[25] A three-dimensional chest CT reconstruction can quantify the contusion volume and help identify individuals at higher risk of ARDS. Patients with contusion volumes of at least 20% have severe disease and are more likely to develop ARDS and pneumonia than patients with contusion volumes of less than 20%.[26]
An ultrasound is a vital bedside imaging tool that can help clinicians quickly identify pulmonary contusion if a chest x-ray or CT cannot be obtained immediately (see Image. Pulmonary Contusion On Ultrasound). The focused assessment with sonography for trauma (FAST) exam is a normal part of the initial trauma assessment but is limited to the pericardium and peritoneum. Extended FAST (E-FAST) includes a chest exam.[27] E-FAST can help expedite management planning for patients with pulmonary contusions.[28]
Electrocardiography (ECG) is indispensable when evaluating patients with blunt chest injuries, with or without suspicion of a pulmonary pathology. Cardiac contusion, which is rapidly fatal, is also likely in such cases. For example, a precordial blow during a sports collision can trigger an arrhythmia such as ventricular fibrillation, resulting in a fatal condition called "commotio cordis."[29]
Treatment / Management
Most pulmonary contusions require supportive therapy until the injury heals. Continuous close monitoring is necessary because contusions can evolve even 24 to 48 hours after trauma. The management goal should be respiratory insufficiency prevention. Patients must be given appropriate pain control to avoid splinting chest muscles and allow lung expansion.
Supportive Care
Postural drainage, suctioning, chest physiotherapy, incentive spirometry, encouraging coughing, and deep breathing help prevent atelectasis. Addressing associated injuries like rib and sternal fractures is also paramount. Pain control can reduce pulmonary morbidity by allowing lung expansion and preventing atelectasis.[30]
Pulmonary contusion is an independent predictor of the need for tracheal intubation in chest trauma.[31] Ventilation settings must be chosen carefully to keep the alveoli patent and recruit more alveoli while preventing barotrauma. Continuous positive airway pressure (CPAP) or bilevel positive airway pressure (BiPAP) may be provided to patients who do not require intubation. (B2)
Prone positioning of the patient with contusion reduces pressure on the diaphragm. Additionally, positioning the contused lung in a non-dependent position helps recruit alveoli. Noninvasive ventilation (NIV) is relatively contraindicated in patients with impaired consciousness, as it can cause gastric distention and aspiration.[32]
Invasive ventilation is required if positive pressure ventilation fails. However, large tidal volumes can increase the risk of barotrauma. Starting with a low tidal volume is recommended.[33]
Diuretics can reduce pulmonary venous resistance and pulmonary capillary hydrostatic pressure. If fluid therapy is required to maintain euvolemia, measuring pulmonary artery pressure can help avoid pulmonary edema.
Surgery
Patients with multiple rib fractures or flail chest may require surgical stabilization to correct pulmonary mechanics. Rib fracture surgery reduces ventilator days in patients with mild-to-moderate pulmonary contusions.[34] Hypoxia refractory to all conventional therapies has been successfully managed by venovenous extracorporeal membrane oxygenation (vv-ECMO).[35]
Differential Diagnosis
The differentials of breathing difficulty after a traumatic injury include the following:
- Pulmonary disorders: lung laceration, pneumonia, hemothorax, pneumothorax, pulmonary edema, pulmonary embolism, transfusion-associated lung injury (TRALI), asthma
- Cardiac conditions: cardiac contusion, myocardial infarction, pneumomediastinum, myocarditis, aortic dissection, cardiac tamponade
- Musculoskeletal pathology: rib fractures, foreign body injury, muscular contusion
- Psychiatric conditions: panic attack, hyperventilation, anxiety disorder
- Systemic disorders: poisoning, anaphylaxis, acidosis
A detailed medical evaluation will help clinicians distinguish these conditions from pulmonary contusions.
Staging
The Murray score for acute lung injury can help assess lung injury severity.[36] This system has four variables: hypoxemia (PaO2/FiO2), atelectasis, lung compliance, and PEEP. Each variable is assigned a score from 0 to 4. The sum of the scores is divided by the number of examined variables. The final score is interpreted as follows:
- 0 - no lung injury
- 0.1 to 2.5 - mild to moderate lung injury
- Greater than 2.5 - lung injury with ARDS
The Murray Score helps clinicians determine the appropriate ventilator settings for managing patients with acute lung injury or ARDS.
Prognosis
Most pulmonary contusions heal within 5 to 7 days with good supportive care. In a study involving 73 patients with pulmonary contusion, 38.4% were diagnosed with pneumonia, while 6.8% developed ARDS. About 52.1% had greater than 20% pulmonary contusion volume.[38] Individuals who recover from severe pulmonary contusions may develop chronic pulmonary disease, manifesting as diminished functional residual capacity.[22] The mortality rate for lung contusions varies from 14% to 40%, depending on the severity of associated injuries.[39]
Complications
Pulmonary contusions may result in pneumonia, ARDS, and respiratory failure. Patients with polytrauma are more likely (78%) to develop ARDS than those with only pulmonary contusions (17%). The leading causes of mortality within the first month of sustaining a pulmonary contusion are ARDS (44.1%) and respiratory infection (26.5%).
Deterrence and Patient Education
Measures that help prevent pulmonary contusions include the following:
- Using seatbelts, airbags, and age-appropriate car seats while driving
- Fall prevention in susceptible patients
- Following workplace safety guidelines
- Using protective gear during sports activities
- Avoiding risky behaviors
These measures will not prevent all pulmonary injuries. Therefore, patients must be reminded to seek medical attention immediately after experiencing chest trauma.
Pearls and Other Issues
The most important points to remember in pulmonary contusion management are the following:
- Patients with pulmonary contusion may present with chest pain, dyspnea, coughing, and hypoxemia. The symptoms may not always be immediately evident. Clinicians should have a high index of suspicion for this condition, especially after significant chest trauma.
- Diagnosis involves a thorough physical examination, chest x-rays, and sometimes CT scans to evaluate the extent and severity of the contusion. Monitoring oxygen levels and lung function is crucial.
- Management focuses on supportive measures to ensure adequate oxygenation and prevent complications. Supportive measures include supplemental oxygen therapy, pain management, and adequate respiratory support.
- Mechanical ventilation might be required in severe cases. Ventilator settings should aim to keep the alveoli patent, maintain adequate oxygenation, and avoid further lung injury. Lower tidal volumes and high positive end-expiratory pressure (PEEP) are commonly used.
- Complications like pneumonia, ARDS, and infections may develop in patients with pulmonary contusions. Patients must be closely monitored so that prompt intervention can be given if these conditions develop.
- Careful fluid management is crucial to prevent worsening of lung function. Excessive fluids can exacerbate lung injury and compromise oxygenation.
- Adequate pain management facilitates deep breathing and prevents atelectasis.
- Managing pulmonary contusion best involves a multidisciplinary team comprised of emergency medicine physicians, intensivists, respiratory therapists, surgeons, and nurses to ensure comprehensive care.
Managing pulmonary contusion should be individualized based on the injury's severity and the patient's baseline health status. Early recognition and prompt intervention can significantly impact outcomes in patients with this condition.
Enhancing Healthcare Team Outcomes
A multidisciplinary team approach is vital in managing pulmonary contusions, especially when dealing with severe or intensive care cases. The key members and their roles are the following:
- Emergency medicine physicians - initiate the evaluation and stabilization of patients with chest trauma. Emergency medicine physicians coordinate initial assessments, order diagnostic tests, and provide immediate interventions to stabilize the patient's condition.
- Trauma surgeons - may evaluate patients and provide surgical interventions in cases of severe trauma leading to pulmonary contusion.
- Intensivists or critical care physicians - manage severe pulmonary contusion cases, especially those requiring intensive care unit (ICU) admission and mechanical ventilation. These providers oversee respiratory support and overall management in the critical care setting.
- Respiratory therapists - manage mechanical ventilation, optimize oxygenation strategies, and assist in initiating ventilator weaning protocols. Respiratory therapists also aid in airway management and pulmonary rehabilitation.
- Radiologists - interpret imaging studies, aiding in diagnosis and guiding treatment decisions.
- Nurses - provide continuous monitoring, administer medications, help manage ventilator settings, ensure patient comfort, and coordinate patient care, especially in the ICU.
- Physical and occupational therapists - assist in early mobilization, chest physiotherapy, and pulmonary rehabilitation to prevent complications and improve overall functional outcomes.
- Pain management specialists - optimize pain control strategies, allowing patients to breathe deeply to prevent atelectasis.
- Nutritionists and dietitians - ensure optimal nutritional support for critically ill individuals to aid in the healing process.
- Social workers and counselors - address patients' psychosocial needs and provide resources that can help during recovery.
Effective collaboration among these multidisciplinary team members is essential for delivering comprehensive care, optimizing treatment strategies, and promoting the best possible outcomes for patients with pulmonary contusion.
Media
(Click Image to Enlarge)
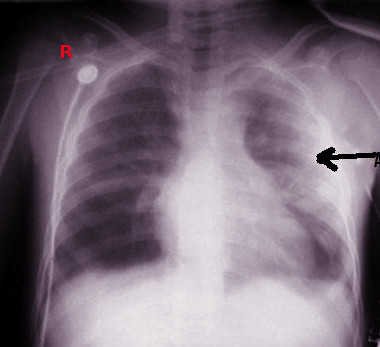
Pulmonary Contusion Radiograph. This image shows a left pulmonary contusion.
Contributed by Steve Bhimji, MS, MD, PhD
(Click Video to Play)
Pulmonary Contusion On Ultrasound. Focal B-lines in a trauma patient are indicative of pulmonary contusions.
Contributed by Ami Kurzweil, MD
(Click Image to Enlarge)
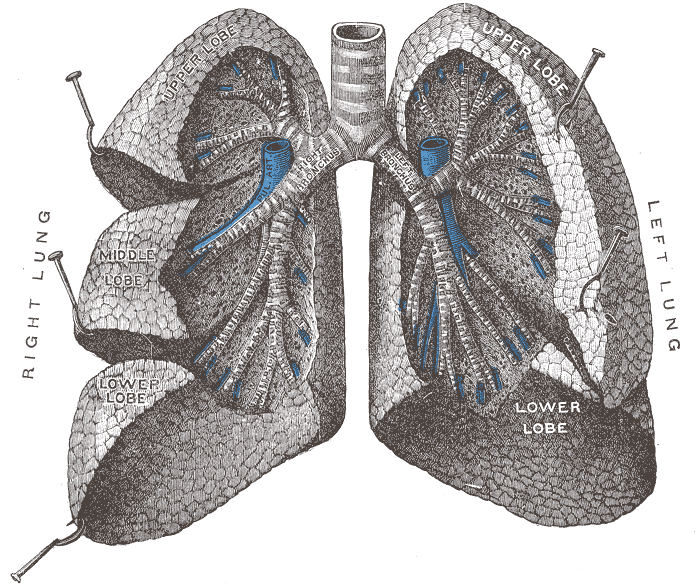
Tracheobronchial Tree, Anterior View. Shown in this illustration are the trachea, right and left main bronchi, lobar bronchi, and segmental bronchi. The lung lobes shown include the right upper, middle, and lower lobes and the left upper and lower lobes.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
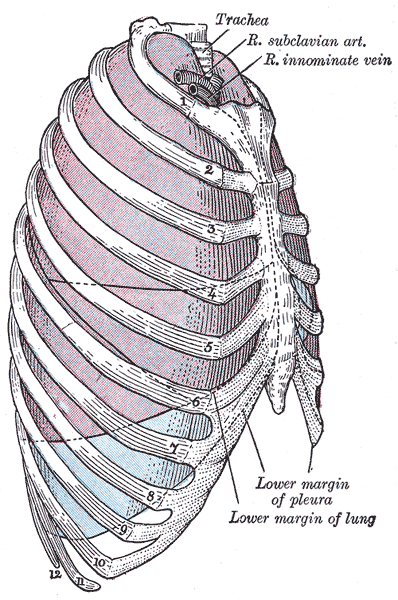
Relationship Of Thoracic Contents And Thoracic Cage Linings. Shown in this lateral-view illustration are the trachea, right subclavian artery, right innominate vein, sternum, ribs, lungs (purple), and pleurae (blue). The lung apices project superiorly in the supraclavicular fossae. The lungs' inferior margins pass anterolaterally from the 6th rib at the midclavicular line to the 8th rib at the midaxillary line. Posteriorly, the inferior lung margin is at the 10th rib at the scapular line (not shown).
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
References
Karmy-Jones R, Jurkovich GJ. Blunt chest trauma. Current problems in surgery. 2004 Mar:41(3):211-380 [PubMed PMID: 15097979]
Cohn SM. Pulmonary contusion: review of the clinical entity. The Journal of trauma. 1997 May:42(5):973-9 [PubMed PMID: 9191684]
Level 3 (low-level) evidenceRendeki S, Molnár TF. Pulmonary contusion. Journal of thoracic disease. 2019 Feb:11(Suppl 2):S141-S151. doi: 10.21037/jtd.2018.11.53. Epub [PubMed PMID: 30906578]
Ullman EA, Donley LP, Brady WJ. Pulmonary trauma emergency department evaluation and management. Emergency medicine clinics of North America. 2003 May:21(2):291-313 [PubMed PMID: 12793615]
Patel S, Yelne P, Gaidhane SA, Kumar S, Acharya S, Shah D, Patel M, Kakde Y. Lightning Strike Presenting as Fatal Lung Contusion: A Case Report. Cureus. 2022 Dec:14(12):e33125. doi: 10.7759/cureus.33125. Epub 2022 Dec 30 [PubMed PMID: 36726903]
Level 3 (low-level) evidenceEkpe EE, Eyo C. Determinants of mortality in chest trauma patients. Nigerian journal of surgery : official publication of the Nigerian Surgical Research Society. 2014 Jan:20(1):30-4. doi: 10.4103/1117-6806.127107. Epub [PubMed PMID: 24665200]
Ziegler DW, Agarwal NN. The morbidity and mortality of rib fractures. The Journal of trauma. 1994 Dec:37(6):975-9 [PubMed PMID: 7996614]
Ganie FA, Lone H, Lone GN, Wani ML, Singh S, Dar AM, Wani NU, Wani SN, Nazeer NU. Lung Contusion: A Clinico-Pathological Entity with Unpredictable Clinical Course. Bulletin of emergency and trauma. 2013 Jan:1(1):7-16 [PubMed PMID: 27162815]
Deng H, Tang TX, Yao Y, Zhang C, Wu H, Li ZW, Tang LS, Chen D, Chang TD, Yang JZ, Luo JL, Dong L, Yang XP, Tang ZH. The incidence, clinical characteristics, and outcome of polytrauma patients with the combination of pulmonary contusion, flail chest and upper thoracic spinal injury. Injury. 2022 Mar:53(3):1073-1080. doi: 10.1016/j.injury.2021.09.053. Epub 2021 Oct 1 [PubMed PMID: 34625240]
van Wessem KJP, Niemeyer MJS, Leenen LPH. Polytrauma patients with severe cervical spine injuries are different than with severe TBI despite similar AIS scores. Scientific reports. 2022 Dec 13:12(1):21538. doi: 10.1038/s41598-022-25809-8. Epub 2022 Dec 13 [PubMed PMID: 36513675]
Sutyak JP, Wohltmann CD, Larson J. Pulmonary contusions and critical care management in thoracic trauma. Thoracic surgery clinics. 2007 Feb:17(1):11-23, v [PubMed PMID: 17650693]
Benhamed A, Ndiaye A, Emond M, Lieutaud T, Boucher V, Gossiome A, Laumon B, Gadegbeku B, Tazarourte K. Road traffic accident-related thoracic trauma: Epidemiology, injury pattern, outcome, and impact on mortality-A multicenter observational study. PloS one. 2022:17(5):e0268202. doi: 10.1371/journal.pone.0268202. Epub 2022 May 6 [PubMed PMID: 35522686]
Level 2 (mid-level) evidenceDoyle JE, Diaz-Gutierrez I. Traumatic sternal fractures: a narrative review. Mediastinum (Hong Kong, China). 2021:5():34. doi: 10.21037/med-21-27. Epub 2021 Dec 25 [PubMed PMID: 35118339]
Level 3 (low-level) evidenceOppenheimer L, Craven KD, Forkert L, Wood LD. Pathophysiology of pulmonary contusion in dogs. Journal of applied physiology: respiratory, environmental and exercise physiology. 1979 Oct:47(4):718-28 [PubMed PMID: 389910]
Level 3 (low-level) evidencePrentice D, Ahrens T. Pulmonary complications of trauma. Critical care nursing quarterly. 1994 Aug:17(2):24-33 [PubMed PMID: 8055358]
Miller DL, Mansour KA. Blunt traumatic lung injuries. Thoracic surgery clinics. 2007 Feb:17(1):57-61, vi [PubMed PMID: 17650697]
Ward PA. Acute lung injury: how the lung inflammatory response works. The European respiratory journal. Supplement. 2003 Sep:44():22s-23s [PubMed PMID: 14582896]
Level 3 (low-level) evidenceRaghavendran K, Davidson BA, Huebschmann JC, Helinski JD, Hutson AD, Dayton MT, Notter RH, Knight PR. Superimposed gastric aspiration increases the severity of inflammation and permeability injury in a rat model of lung contusion. The Journal of surgical research. 2009 Aug:155(2):273-82. doi: 10.1016/j.jss.2008.08.020. Epub 2008 Sep 16 [PubMed PMID: 19515386]
Level 3 (low-level) evidenceAllen GS, Cox CS Jr. Pulmonary contusion in children: diagnosis and management. Southern medical journal. 1998 Dec:91(12):1099-106 [PubMed PMID: 9853720]
Moseley RV, Vernick JJ, Doty DB. Response to blunt chest injury: a new experimental model. The Journal of trauma. 1970 Aug:10(8):673-83 [PubMed PMID: 5451078]
Level 3 (low-level) evidenceGarzon AA, Seltzer B, Karlson KE. Physiopathology of crushed chest injuries. Annals of surgery. 1968 Jul:168(1):128-36 [PubMed PMID: 5673189]
Allen GS, Coates NE. Pulmonary contusion: a collective review. The American surgeon. 1996 Nov:62(11):895-900 [PubMed PMID: 8895709]
Miller LA. Chest wall, lung, and pleural space trauma. Radiologic clinics of North America. 2006 Mar:44(2):213-24, viii [PubMed PMID: 16500204]
Kaewlai R, Chatpuwaphat J, Butnian K, Thusneyapan K, Panrong N, Lertpipopmetha W, Wongpongsalee T. Thoracic Inlet in Cervical Spine CT of Blunt Trauma Patients: Prevalence of Pathologies and Importance of CT Interpretation. Tomography (Ann Arbor, Mich.). 2022 Nov 19:8(6):2772-2783. doi: 10.3390/tomography8060231. Epub 2022 Nov 19 [PubMed PMID: 36412690]
Level 2 (mid-level) evidenceSchild HH, Strunk H, Weber W, Stoerkel S, Doll G, Hein K, Weitz M. Pulmonary contusion: CT vs plain radiograms. Journal of computer assisted tomography. 1989 May-Jun:13(3):417-20 [PubMed PMID: 2723172]
Level 3 (low-level) evidenceMiller PR, Croce MA, Bee TK, Qaisi WG, Smith CP, Collins GL, Fabian TC. ARDS after pulmonary contusion: accurate measurement of contusion volume identifies high-risk patients. The Journal of trauma. 2001 Aug:51(2):223-8; discussion 229-30 [PubMed PMID: 11493778]
Level 2 (mid-level) evidenceBloom BA, Gibbons RC. Focused Assessment With Sonography for Trauma. StatPearls. 2024 Jan:(): [PubMed PMID: 29261902]
Planquart F, Marcaggi E, Blondonnet R, Clovet O, Bobbia X, Boussat B, Pottecher J, Gauss T, Zieleskiewicz L, Bouzat P. Appropriateness of Initial Course of Action in the Management of Blunt Trauma Based on a Diagnostic Workup Including an Extended Ultrasonography Scan. JAMA network open. 2022 Dec 1:5(12):e2245432. doi: 10.1001/jamanetworkopen.2022.45432. Epub 2022 Dec 1 [PubMed PMID: 36477480]
Frishman WH, Alpert JS. Commotio Cordis and the Triumph of Out-of-Hospital Cardiopulmonary Resuscitation. The American journal of medicine. 2023 May:136(5):401-402. doi: 10.1016/j.amjmed.2023.01.007. Epub 2023 Jan 31 [PubMed PMID: 36736646]
Thomas KP, Sainudeen S, Jose S, Nadhari MY, Macaire PB. Ultrasound-Guided Parasternal Block Allows Optimal Pain Relief and Ventilation Improvement After a Sternal Fracture. Pain and therapy. 2016 Jun:5(1):115-22. doi: 10.1007/s40122-016-0050-5. Epub 2016 Mar 21 [PubMed PMID: 27001634]
Reitano E, Gavelli F, Iannantuoni G, Fattori S, Airoldi C, Matranga S, Cioffi SPB, Ingala S, Virdis F, Rizzo M, Marcomini N, Motta A, Spota A, Maestrone M, Ragozzino R, Altomare M, Castello LM, Della Corte F, Vaschetto R, Avanzi GC, Chiara O, Cimbanassi S. In-Hospital Predictors of Need for Ventilatory Support and Mortality in Chest Trauma: A Multicenter Retrospective Study. Journal of clinical medicine. 2023 Jan 16:12(2):. doi: 10.3390/jcm12020714. Epub 2023 Jan 16 [PubMed PMID: 36675639]
Level 2 (mid-level) evidenceGong Y, Sankari A. Noninvasive Ventilation. StatPearls. 2024 Jan:(): [PubMed PMID: 35201716]
Hickey SM, Giwa AO. Mechanical Ventilation. StatPearls. 2024 Jan:(): [PubMed PMID: 30969564]
Van Wijck SFM, Pieracci FM, Smith EF, Madden K, Moore EE, Wijffels MME, Werner NL. Rib fixation in patients with severe rib fractures and pulmonary contusions: Is it safe? The journal of trauma and acute care surgery. 2022 Dec 1:93(6):721-726. doi: 10.1097/TA.0000000000003790. Epub 2022 Sep 19 [PubMed PMID: 36121283]
Dagod G, Ramin S, Solovei L, Capdevila X, Charbit J. A combined management with vv-ECMO and independent lung ventilation for asymmetric chest trauma. General thoracic and cardiovascular surgery. 2021 May:69(5):902-905. doi: 10.1007/s11748-021-01587-4. Epub 2021 Jan 13 [PubMed PMID: 33439375]
Nikischin W, Gerhardt T, Everett R, Bancalari E. A new method to analyze lung compliance when pressure-volume relationship is nonlinear. American journal of respiratory and critical care medicine. 1998 Oct:158(4):1052-60 [PubMed PMID: 9769260]