Introduction
Spinal immobilization with a backboard and cervical collar for patients with suspected spine injury became common practice in the 1960s. The increase in automobile accidents drove this decision as automobiles became more commonplace, and a position paper was published by the American Academy of Orthopedics endorsing its use without evidence that spinal immobilization improved outcomes.[1][2][3][4][5][6][7][8] Spinal immobilization included a cervical collar and a rigid backboard with secured straps. Recent studies assessing the validity of spinal immobilization raised concern for harm instead of better outcomes). In the early 2010s, the common practice moved to spinal motion restriction to replace the common use of spinal immobilization.[1] In 2019, a retrospective observational study from the University of Arizona showed no significant increase in spinal cord injury after transitioning from a spinal immobilization protocol to 1 of spinal motion restrictions.[9]
Indications
A joint position paper between the American College of Surgeons Committee on Trauma (ACS-COT), American College of Emergency Physicians (ACEP), and the National Association of Emergency Medicine Physicians (NAEMSP) in 2018 outlined the uniform recommendations for spinal motion restriction in the care of trauma patients.[1] The indications for patients who have experienced blunt trauma are summarized in the table (see Table. Indications for Spinal Motion Restriction). Patients with none of the identified indications should not undergo spinal motion restriction due to the potential for harm by being placed in a cervical collar or backboard. In the pediatric population, there is no indication based on age alone for using spinal motion restriction.[10][11] Young patients can present a challenge to providers due to communication issues. A retrospective review completed by Hale et al of 2,972 pre-elementary trauma patients showed that CT scans were not necessary for patients less than 5 years old without clinical findings on the exam. In addition to the criteria listed in the table, torticollis indicates spinal motion restriction (particularly cervical collar placement) in pediatric patients.[12]
Issues of Concern
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Issues of Concern
Contraindications
Spinal motion restriction should not be used in the patient with penetrating trauma. In their 2010 publication, Haut et al reviewed 45,284 patients who had entered the National Trauma Data Bank (NTDB). They found that patients with penetrating trauma who underwent spinal immobilization in the field, defined as placement of a cervical collar or longboard, had mortality rates twice as high as those who did not.[13] The Eastern Association for the Surgery of Trauma (EAST) performed a systematic review of 24 studies in 2018 that showed no benefit to spinal immobilization in either mortality or neurologic recovery, even in those with a direct neck injury.[2]
Complications
The earlier ubiquitous use of the backboard revealed several significant complications, leading to an evidence-based transition from immobilization with a backboard to the current use of spinal motion restriction. The forceful strapping of patients against a rigid backboard is incompatible with the natural curvature of the spine, and such restriction may increase unwanted flexion, extension, and rotation. This effect is more pronounced in populations such as the elderly or those with ankylosing spondylitis who develop marked kyphosis or lordosis.[3] Moving these patients onto a stretcher and off the backboard as soon as possible is preferable. Even when moved to a cot, additional padding with towels or pillows is often required to maintain the patient’s natural alignment and prevent further injury. Similar considerations should be taken with children to prevent excess cervical spine flexion due to high variation in head-to-body size.
In a 2014 systematic review in The Journal of Trauma and Acute Care Surgery, 5 studies showed increased pain scores following immobilization.[4] Patients placed into strict immobilization with a backboard are at higher risk for developing pressure ulcers in as little as thirty minutes.[6] In 2013, a review by Cooney et al showed that patients spent an average of 1 hour secured to a backboard after undergoing spinal immobilization in the field.[12] Even without the straps, patients should not be left on a hard backboard during transport to the hospital to prevent pain and ulcer development. Spinal motion restriction allows for neutral alignment on a cot or stretcher, but providers should pay attention to providing padding or support where needed. Providers should monitor respiratory status closely when utilizing the backboard as a movement tool from extrication to ambulance. Studies have shown significant respiratory restriction in healthy patients who were strapped to a backboard with cervical collars. This restriction was greater in elderly kyphotic patients placed in a cervical collar.[7][8] Patients with significant blunt chest and neck trauma may already have diminished respiratory capacity due to injuries that could worsen with further constriction.
Clinical Significance
Spinal motion restriction is the use of a cervical collar and cot to maintain neutral alignment of the spine during transport of the patient with concern for spinal injury. The goal is to reduce excessive movement of the spine that may worsen existing spinal trauma and neurologic deficits. While backboards may work for the initial extrication and movement of a patient, it is preferable to bring the cot or stretcher to the ambulatory patient and instruct them to lie down. Do not perform a vertical backboard takedown. The backboard requires removal as soon as possible before being transported by emergency medical services to the hospital. Recent studies suggest that full spinal immobilization does not limit motion during prehospital transportation as much as previously thought. While this was most notable in the non-compliant patient, the increased movement was seen in the compliant patient population.[14]Not all patients can lie flat on their back on a stretcher. An alert patient with nausea and vomiting may need to have the head of the bed elevated or be rolled on their side to avoid aspiration. If a patient requires intubation, elevating the head of the bed has been demonstrated to improve oxygenation and hemodynamic stability.[15] In an altered patient with head trauma, providers should consider elevating the head of the bed to decrease intracranial pressure. If a patient needs the head of their bed raised, spinal motion restriction requires support through the head, neck, and torso; this is impossible with a patient on a backboard.
While most spinal injuries are due to high-force mechanisms, special care is necessary for geriatric patients (age 65 and older) who may present without typical physical exam findings (ie, midline neck pain) after a ground-level fall. A 2013 retrospective review of 12,805 geriatric trauma patients found cervical spine fractures in over half of geriatric patients with ground-level falls. Overall, geriatric patients were more likely to sustain upper cervical fractures than non-geriatric patients, and researchers found ground-level falls to cause both isolated cervical fractures and significant intracranial pathology.[16] Providers should have a high index of suspicion for significant injury in this population, even with a low force mechanism.
Media
(Click Image to Enlarge)
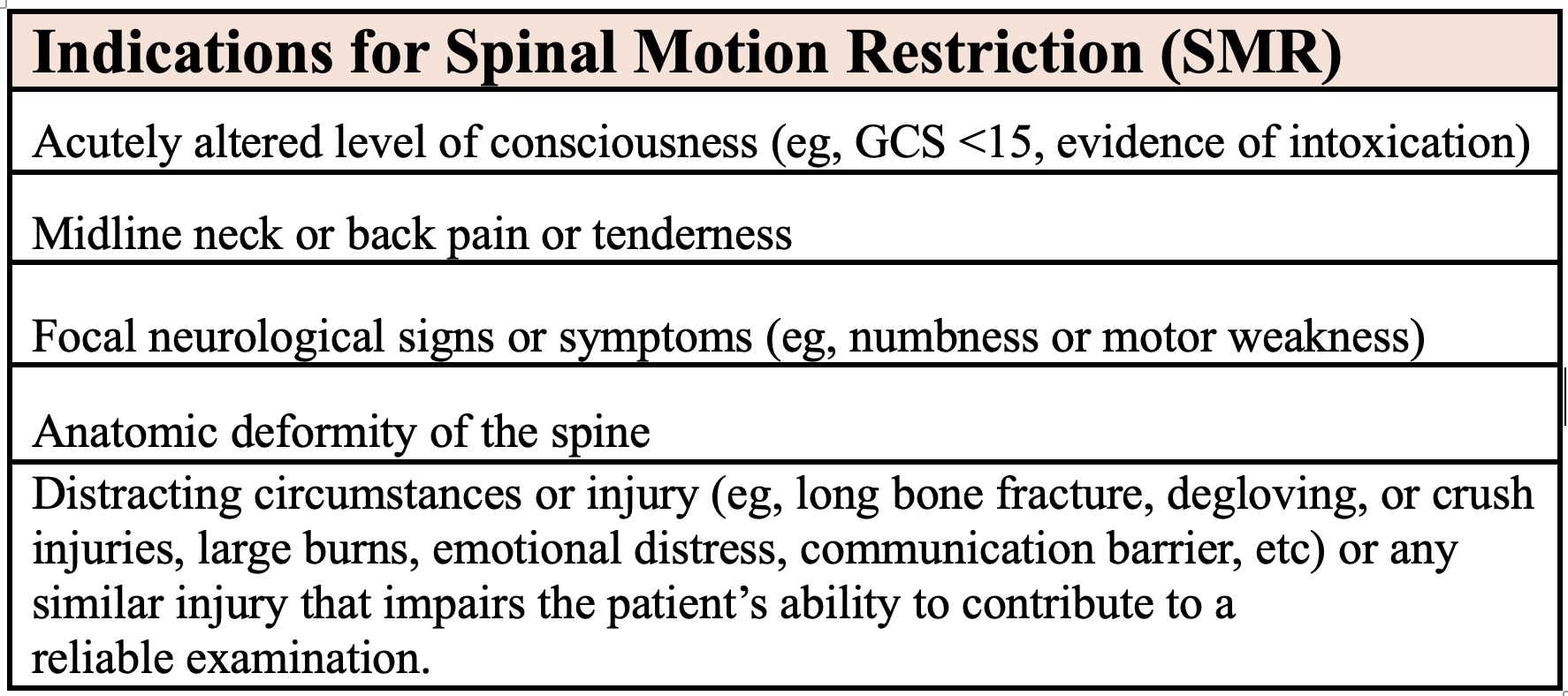
Indications for Spinal Motion Restriction
Contributed by E Kane, MD
References
White CC 4th, Domeier RM, Millin MG, Standards and Clinical Practice Committee, National Association of EMS Physicians. EMS spinal precautions and the use of the long backboard - resource document to the position statement of the National Association of EMS Physicians and the American College of Surgeons Committee on Trauma. Prehospital emergency care. 2014 Apr-Jun:18(2):306-14. doi: 10.3109/10903127.2014.884197. Epub 2014 Feb 21 [PubMed PMID: 24559236]
Velopulos CG, Shihab HM, Lottenberg L, Feinman M, Raja A, Salomone J, Haut ER. Prehospital spine immobilization/spinal motion restriction in penetrating trauma: A practice management guideline from the Eastern Association for the Surgery of Trauma (EAST). The journal of trauma and acute care surgery. 2018 May:84(5):736-744. doi: 10.1097/TA.0000000000001764. Epub [PubMed PMID: 29283970]
Papadopoulos MC, Chakraborty A, Waldron G, Bell BA. Lesson of the week: exacerbating cervical spine injury by applying a hard collar. BMJ (Clinical research ed.). 1999 Jul 17:319(7203):171-2 [PubMed PMID: 10406758]
Level 3 (low-level) evidenceHam HW,Schoonhoven LL,Schuurmans MM,Leenen LL, Pressure ulcer development in trauma patients with suspected spinal injury; the influence of risk factors present in the Emergency Department. International emergency nursing. 2017 Jan; [PubMed PMID: 27450044]
Edlich RF, Mason SS, Vissers RJ, Gubler KD, Thacker JG, Pharr P, Anderson M, Long WB 3rd. Revolutionary advances in enhancing patient comfort on patients transported on a backboard. The American journal of emergency medicine. 2011 Feb:29(2):181-6. doi: 10.1016/j.ajem.2009.08.027. Epub 2010 Mar 25 [PubMed PMID: 20825784]
Level 3 (low-level) evidenceSparke A, Voss S, Benger J. The measurement of tissue interface pressures and changes in jugular venous parameters associated with cervical immobilisation devices: a systematic review. Scandinavian journal of trauma, resuscitation and emergency medicine. 2013 Dec 3:21():81. doi: 10.1186/1757-7241-21-81. Epub 2013 Dec 3 [PubMed PMID: 24299024]
Level 1 (high-level) evidenceTotten VY, Sugarman DB. Respiratory effects of spinal immobilization. Prehospital emergency care. 1999 Oct-Dec:3(4):347-52 [PubMed PMID: 10534038]
Level 1 (high-level) evidenceWalsh M,Grant T,Mickey S, Lung function compromised by spinal immobilization. Annals of emergency medicine. 1990 May; [PubMed PMID: 2331117]
Level 3 (low-level) evidenceCastro-Marin F, Gaither JB, Rice AD, N Blust R, Chikani V, Vossbrink A, Bobrow BJ. Prehospital Protocols Reducing Long Spinal Board Use Are Not Associated with a Change in Incidence of Spinal Cord Injury. Prehospital emergency care. 2020 May-Jun:24(3):401-410. doi: 10.1080/10903127.2019.1645923. Epub 2019 Aug 14 [PubMed PMID: 31348691]
Pieretti-Vanmarcke R, Velmahos GC, Nance ML, Islam S, Falcone RA Jr, Wales PW, Brown RL, Gaines BA, McKenna C, Moore FO, Goslar PW, Inaba K, Barmparas G, Scaife ER, Metzger RR, Brockmeyer DL, Upperman JS, Estrada J, Lanning DA, Rasmussen SK, Danielson PD, Hirsh MP, Consani HF, Stylianos S, Pineda C, Norwood SH, Bruch SW, Drongowski R, Barraco RD, Pasquale MD, Hussain F, Hirsch EF, McNeely PD, Fallat ME, Foley DS, Iocono JA, Bennett HM, Waxman K, Kam K, Bakhos L, Petrovick L, Chang Y, Masiakos PT. Clinical clearance of the cervical spine in blunt trauma patients younger than 3 years: a multi-center study of the american association for the surgery of trauma. The Journal of trauma. 2009 Sep:67(3):543-9; discussion 549-50. doi: 10.1097/TA.0b013e3181b57aa1. Epub [PubMed PMID: 19741398]
Level 2 (mid-level) evidenceHale DF, Fitzpatrick CM, Doski JJ, Stewart RM, Mueller DL. Absence of clinical findings reliably excludes unstable cervical spine injuries in children 5 years or younger. The journal of trauma and acute care surgery. 2015 May:78(5):943-8. doi: 10.1097/TA.0000000000000603. Epub [PubMed PMID: 25909413]
Cooney DR,Wallus H,Asaly M,Wojcik S, Backboard time for patients receiving spinal immobilization by emergency medical services. International journal of emergency medicine. 2013 Jun 20; [PubMed PMID: 23786995]
Haut ER, Kalish BT, Efron DT, Haider AH, Stevens KA, Kieninger AN, Cornwell EE 3rd, Chang DC. Spine immobilization in penetrating trauma: more harm than good? The Journal of trauma. 2010 Jan:68(1):115-20; discussion 120-1. doi: 10.1097/TA.0b013e3181c9ee58. Epub [PubMed PMID: 20065766]
McDonald N, Kriellaars D, Weldon E, Pryce R. Head-Neck Motion in Prehospital Trauma Patients under Spinal Motion Restriction: A Pilot Study. Prehospital emergency care. 2021 Jan-Feb:25(1):117-124. doi: 10.1080/10903127.2020.1727591. Epub 2020 Mar 18 [PubMed PMID: 32045315]
Level 3 (low-level) evidenceSpooner AJ, Corley A, Sharpe NA, Barnett AG, Caruana LR, Hammond NE, Fraser JF. Head-of-bed elevation improves end-expiratory lung volumes in mechanically ventilated subjects: a prospective observational study. Respiratory care. 2014 Oct:59(10):1583-9. doi: 10.4187/respcare.02733. Epub 2014 May 20 [PubMed PMID: 24847096]
Level 2 (mid-level) evidenceWang H,Coppola M,Robinson RD,Scribner JT,Vithalani V,de Moor CE,Gandhi RR,Burton M,Delaney KA, Geriatric Trauma Patients With Cervical Spine Fractures due to Ground Level Fall: Five Years Experience in a Level One Trauma Center. Journal of clinical medicine research. 2013 Apr; [PubMed PMID: 23519239]