Introduction
Hip pain is a common clinical complaint and a source of disability with an incidence of 12 to 15 percent among all adults over the age of 60 years.[1][2] Radiographic hip osteoarthritis affects 27% of adults above the age of 45 years.[3] A lifetime risk of 25% is seen in those who are older than 85 years of age and with a 10% lifetime risk for eventual total hip replacement.[4][5] Osteoarthritis of the hip involves a progressive loss of articular cartilage. Subchondral cysts, osteophyte formation, and synovial inflammation can subsequently develop. Therapeutic hip joint injection with corticosteroids, hyaluronic acid, and plasma-rich platelets have formed the cornerstone of non-surgical management of hip pain.
The important aspects of a fluoroscopic guided hip joint injection include:
- Minimize patient discomfort
- Maintain patient safety
- Maintain proper needle technique in accessing the intraarticular joint space
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
The hip joint is composed of the articulation of the femoral head and the acetabulum. The femoroacetabular joint is a ball-in-socket synovial joint and is stabilized by accessory elements that include different ligament restraints.[6] The complex biomechanics of this joint allows for a wide range of activities that include maintaining a steady gait, rising from a seated position, and adequately ambulating.[7] The ileum, pubis, and ischium constitute the pelvis. Together they form the acetabular socket, which articulates with the femoral head. At any given time, approximately 40% of the femoral head is covered by the acetabulum.[8] The labrum provides additional stability and is made up of a rim of collagen fibers.[9] The pubofemoral, ischiofemoral, and iliofemoral ligaments form the joint capsule providing additional stability to the hip joint.[10] Hip osteoarthritis is deterioration and loss of articular cartilage of the femoroacetabular joint. Subchondral bone, the associated ligaments of the hip joint, and the synovium are also progressively affected in varying degrees. The pathogenesis of osteoarthritis is complex; however, it is generally accepted that various biomechanical factors and environmental factors, as well as a contribution of general wear-and-tear through time, play a role in the development of osteoarthritis.
Indications
The indications for access to the hip joint include:
- Alleviation of pain
- Diagnostic evaluation to determine the source of pain
- Joint aspiration
Contraindications
Absolute contraindications include, but are not limited to:
- Septic arthritis
- Cellulitis at or near the skin entrance of the injection needle
- Bacteremia
- Acute fracture
- Anaphylaxis/allergy to injected therapeutic agents
Equipment
Equipment, including needle gauge, and pharmacotherapeutic mixtures vary institutionally and can be operator-specific. The following list includes a brief overview of possible equipment used for the described procedure.
Potential equipment for a femoroacetabular joint injection include:
- Fenestrated drape or towel drapes
- Fluoroscopy machine
- 1 milliliter (mL) to 3 mL of 1% lidocaine hydrochloride for local anesthesia
- 23-gauge spinal needle
- 2 mL to 4 mL of iodinated contrast
- For corticosteroid injections: Approximately 3 mL of a mixture of 1% lidocaine (2 mL) and triamcinolone 40 mg/mL (1 mL)
Personnel
Personnel includes:
- Clinician performing the injection
- A radiology technologist trained in using the fluoroscopy machine
Preparation
A thorough discussion with a patient prior to the procedure includes the following:
- A detailed explanation of the procedure
- The expected level of discomfort
- A thorough evaluation of the skin entry site
- Prior medical conditions or surgeries that might affect the procedure, to include joint prosthesis
- Potential diagnoses resulting from the procedure
- Potential complications of the procedure
Prior to beginning the fluoroscopic procedure, appropriate lead aprons are worn by all personnel involved. The patient is placed in a comfortable supine position. The patient's lower extremity is placed in either neutral position or is slightly internally rotated to around 10 degrees. Small weights can be placed lateral to both feet to limit motion and to maintain a neutral leg position throughout the procedure. A brief fluoroscopic image is obtained with a metallic marker stick overlying the lateral aspect of the femoral head-neck junction in order for the operator to visualize and plan the proposed needle trajectory. The skin is then marked at the proposed site of entry.
Technique or Treatment
After the skin is marked, the local subcutaneous soft tissues are anesthetized with 1 mL to 3 mL of 1% lidocaine hydrochloride for local anesthesia. A 23-gauge 3.5-inch spinal needle is then used with a stylet in place with an anterior/vertical approach entry through the soft tissues until the femoral head-neck junction cortex is reached. Intermittent fluoroscopy allows for careful centering of the needle hub over the needle tip to ensure a precise perpendicular approach into the joint space. The needle is slightly retracted to avoid immediate termination within the femoral neck hyaline cartilage. The stylet is removed, and a small volume of anesthetic is then injected to ensure low-pressure intra-articular placement and anesthetization of the cortical surface. A test contrast injection with approximately 0.5 mL to 2 mL of contrast ensures that the needle does not terminate within an adjacent bursa and is truly intra-articular. A syringe containing the corticosteroid with or without a connecting tube is then attached to the 23-gauge needle, and the corticosteroid is subsequently injected into the joint.
Complications
Complications are rare and include:
- Exacerbation of baseline pain, especially the night of the procedure which may be related to bland synovitis
- Allergic reaction
- Small vessel injury
The patient's prior imaging should be reviewed to assess for aberrant/variant anatomy.
Clinical Significance
Hip pain is one of the most common outpatient musculoskeletal complaints with a reported prevalence of 19% for those above the age of 65 years.[11] An estimated 27 million individuals are affected by hip pain.[12] Hip pain and related dysfunction have a significant impact on the quality of life. Underlying inflammation from osteoarthrosis related to aging and trauma usually underlies the pathogenesis of acute and chronic pain of the femoroacetabular joint. Older age, obesity, genetics, and occupations involving heavy impact activities and heavy manual work are predisposing factors.[13][14][15][16]
Nonpharmacological therapies include low impact activity exercise regimens such as aquatic exercises.[17][18] Early osteoarthritis is also often treated with physical therapy.[19] Weight reduction, hot/cold treatment, and assistive devices such as crutches also play a role in the management of hip pain.[20][21] Intraarticular injections with hyaluronic acids, corticosteroids, and platelet-rich plasma provide short term relief and play a role as an adjuvant therapy to other non-operative modalities.[22] A 2016 systematic review found that intraarticular corticosteroid injection of the hip joint provided short term pain relief in patients affected by osteoarthritis-related pain.[23] Data involving pain relief with hyaluronic acid and platelet-rich plasma vary, but also generally demonstrate efficacy.[24][21] Fluoroscopic guidance for injections described in this article helps in avoiding critical structures of the hip joint with enhanced needle guidance.
Enhancing Healthcare Team Outcomes
The role of a radiology technologist is exceptionally important in helping the operator during the procedure. Patient comfort is critical in properly performing the procedure as significant patient movement can affect satisfactory targeting of the hip joint. Movement can also affect needle trajectory with a potential injury of the femoral neuro-vasculature. The technologist plays an important role in assisting in fluoroscopic image acquisition. Documentation of immediate pain relief is important for the referring provider, as this can help further manage treatment.
Media
(Click Image to Enlarge)

A small amount of iodinated contrast is injected into the femoroacetabular joint to ensure appropriate needle entry into the joint space. Contributed by Dr.Dawood Tafti
(Click Image to Enlarge)

Initial fluoroscopic visualization of the hip joint. The metallic marker denotes the femoral head-neck junction as the target site for injection Contributed by Dr.Dawood Tafti
(Click Image to Enlarge)

A vertical approach to hip joint injection is demonstrated. Contributed by Dr.Dawood Tafti
(Click Image to Enlarge)
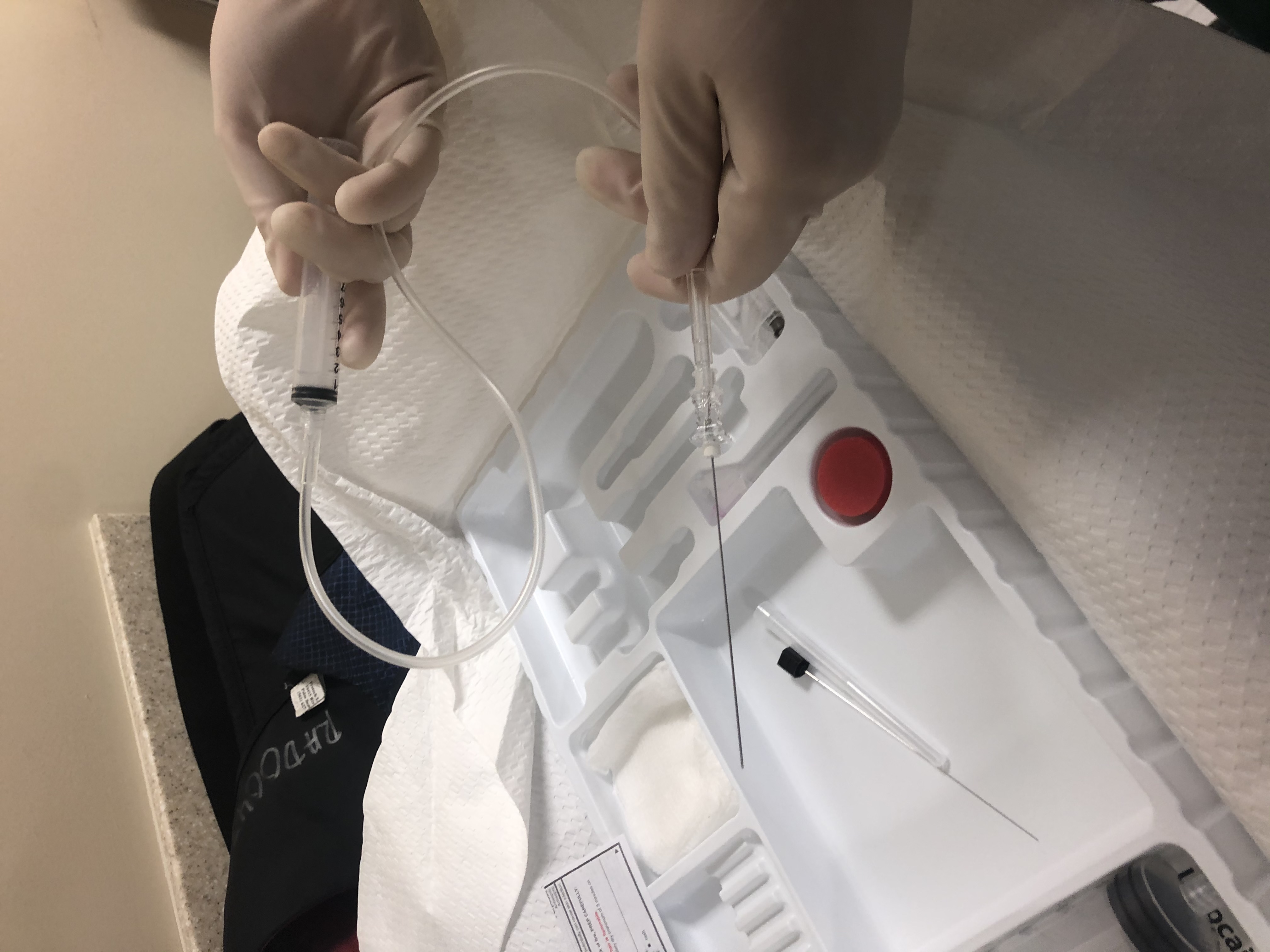
Injection equipment with a spinal needle, supportive tubing, and a syringe. Contributed by Dr.Dawood Tafti
References
Christmas C, Crespo CJ, Franckowiak SC, Bathon JM, Bartlett SJ, Andersen RE. How common is hip pain among older adults? Results from the Third National Health and Nutrition Examination Survey. The Journal of family practice. 2002 Apr:51(4):345-8 [PubMed PMID: 11978258]
Level 2 (mid-level) evidenceCecchi F, Mannoni A, Molino-Lova R, Ceppatelli S, Benvenuti E, Bandinelli S, Lauretani F, Macchi C, Ferrucci L. Epidemiology of hip and knee pain in a community based sample of Italian persons aged 65 and older. Osteoarthritis and cartilage. 2008 Sep:16(9):1039-46. doi: 10.1016/j.joca.2008.01.008. Epub 2008 Mar 17 [PubMed PMID: 18343164]
Level 2 (mid-level) evidenceJordan JM, Helmick CG, Renner JB, Luta G, Dragomir AD, Woodard J, Fang F, Schwartz TA, Nelson AE, Abbate LM, Callahan LF, Kalsbeek WD, Hochberg MC. Prevalence of hip symptoms and radiographic and symptomatic hip osteoarthritis in African Americans and Caucasians: the Johnston County Osteoarthritis Project. The Journal of rheumatology. 2009 Apr:36(4):809-15. doi: 10.3899/jrheum.080677. Epub 2009 Mar 13 [PubMed PMID: 19286855]
Murphy LB, Helmick CG, Schwartz TA, Renner JB, Tudor G, Koch GG, Dragomir AD, Kalsbeek WD, Luta G, Jordan JM. One in four people may develop symptomatic hip osteoarthritis in his or her lifetime. Osteoarthritis and cartilage. 2010 Nov:18(11):1372-9. doi: 10.1016/j.joca.2010.08.005. Epub 2010 Aug 14 [PubMed PMID: 20713163]
Culliford DJ, Maskell J, Kiran A, Judge A, Javaid MK, Cooper C, Arden NK. The lifetime risk of total hip and knee arthroplasty: results from the UK general practice research database. Osteoarthritis and cartilage. 2012 Jun:20(6):519-24. doi: 10.1016/j.joca.2012.02.636. Epub 2012 Mar 3 [PubMed PMID: 22395038]
Glenister R, Sharma S. Anatomy, Bony Pelvis and Lower Limb, Hip. StatPearls. 2023 Jan:(): [PubMed PMID: 30252275]
Bowman KF Jr, Fox J, Sekiya JK. A clinically relevant review of hip biomechanics. Arthroscopy : the journal of arthroscopic & related surgery : official publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 2010 Aug:26(8):1118-29. doi: 10.1016/j.arthro.2010.01.027. Epub [PubMed PMID: 20678712]
Gunay C, Atalar H, Dogruel H, Yavuz OY, Uras I, Sayli U. Correlation of femoral head coverage and Graf alpha angle in infants being screened for developmental dysplasia of the hip. International orthopaedics. 2009 Jun:33(3):761-4. doi: 10.1007/s00264-008-0570-7. Epub 2008 May 21 [PubMed PMID: 18493759]
Level 2 (mid-level) evidenceBonner TF, Colbrunn RW, Bottros JJ, Mutnal AB, Greeson CB, Klika AK, van den Bogert AJ, Barsoum WK. The contribution of the acetabular labrum to hip joint stability: a quantitative analysis using a dynamic three-dimensional robot model. Journal of biomechanical engineering. 2015 Jun:137(6):061012. doi: 10.1115/1.4030012. Epub 2015 Apr 23 [PubMed PMID: 25759977]
Hidaka E, Aoki M, Izumi T, Suzuki D, Fujimiya M. Ligament strain on the iliofemoral, pubofemoral, and ischiofemoral ligaments in cadaver specimens: biomechanical measurement and anatomical observation. Clinical anatomy (New York, N.Y.). 2014 Oct:27(7):1068-75. doi: 10.1002/ca.22425. Epub 2014 Jun 10 [PubMed PMID: 24913440]
Dawson J, Linsell L, Zondervan K, Rose P, Randall T, Carr A, Fitzpatrick R. Epidemiology of hip and knee pain and its impact on overall health status in older adults. Rheumatology (Oxford, England). 2004 Apr:43(4):497-504 [PubMed PMID: 14762225]
Level 2 (mid-level) evidenceBarbour KE, Helmick CG, Boring M, Brady TJ. Vital Signs: Prevalence of Doctor-Diagnosed Arthritis and Arthritis-Attributable Activity Limitation - United States, 2013-2015. MMWR. Morbidity and mortality weekly report. 2017 Mar 10:66(9):246-253. doi: 10.15585/mmwr.mm6609e1. Epub 2017 Mar 10 [PubMed PMID: 28278145]
Muraki S, Akune T, Oka H, Ishimoto Y, Nagata K, Yoshida M, Tokimura F, Nakamura K, Kawaguchi H, Yoshimura N. Incidence and risk factors for radiographic knee osteoarthritis and knee pain in Japanese men and women: a longitudinal population-based cohort study. Arthritis and rheumatism. 2012 May:64(5):1447-56. doi: 10.1002/art.33508. Epub [PubMed PMID: 22135156]
Oliveria SA, Felson DT, Cirillo PA, Reed JI, Walker AM. Body weight, body mass index, and incident symptomatic osteoarthritis of the hand, hip, and knee. Epidemiology (Cambridge, Mass.). 1999 Mar:10(2):161-6 [PubMed PMID: 10069252]
Level 2 (mid-level) evidenceMacGregor AJ, Antoniades L, Matson M, Andrew T, Spector TD. The genetic contribution to radiographic hip osteoarthritis in women: results of a classic twin study. Arthritis and rheumatism. 2000 Nov:43(11):2410-6 [PubMed PMID: 11083262]
Kujala UM, Kaprio J, Sarna S. Osteoarthritis of weight bearing joints of lower limbs in former élite male athletes. BMJ (Clinical research ed.). 1994 Jan 22:308(6923):231-4 [PubMed PMID: 8111258]
Fransen M, McConnell S, Hernandez-Molina G, Reichenbach S. Exercise for osteoarthritis of the hip. The Cochrane database of systematic reviews. 2014 Apr 22:(4):CD007912. doi: 10.1002/14651858.CD007912.pub2. Epub 2014 Apr 22 [PubMed PMID: 24756895]
Level 1 (high-level) evidenceBartels EM, Juhl CB, Christensen R, Hagen KB, Danneskiold-Samsøe B, Dagfinrud H, Lund H. Aquatic exercise for the treatment of knee and hip osteoarthritis. The Cochrane database of systematic reviews. 2016 Mar 23:3(3):CD005523. doi: 10.1002/14651858.CD005523.pub3. Epub 2016 Mar 23 [PubMed PMID: 27007113]
Level 1 (high-level) evidenceZhang W, Doherty M, Arden N, Bannwarth B, Bijlsma J, Gunther KP, Hauselmann HJ, Herrero-Beaumont G, Jordan K, Kaklamanis P, Leeb B, Lequesne M, Lohmander S, Mazieres B, Martin-Mola E, Pavelka K, Pendleton A, Punzi L, Swoboda B, Varatojo R, Verbruggen G, Zimmermann-Gorska I, Dougados M, EULAR Standing Committee for International Clinical Studies Including Therapeutics (ESCISIT). EULAR evidence based recommendations for the management of hip osteoarthritis: report of a task force of the EULAR Standing Committee for International Clinical Studies Including Therapeutics (ESCISIT). Annals of the rheumatic diseases. 2005 May:64(5):669-81 [PubMed PMID: 15471891]
Level 1 (high-level) evidenceCurtis GL, Chughtai M, Khlopas A, Newman JM, Khan R, Shaffiy S, Nadhim A, Bhave A, Mont MA. Impact of Physical Activity in Cardiovascular and Musculoskeletal Health: Can Motion Be Medicine? Journal of clinical medicine research. 2017 May:9(5):375-381. doi: 10.14740/jocmr3001w. Epub 2017 Apr 1 [PubMed PMID: 28392856]
Hochberg MC, Altman RD, April KT, Benkhalti M, Guyatt G, McGowan J, Towheed T, Welch V, Wells G, Tugwell P, American College of Rheumatology. American College of Rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip, and knee. Arthritis care & research. 2012 Apr:64(4):465-74 [PubMed PMID: 22563589]
da Costa BR, Reichenbach S, Keller N, Nartey L, Wandel S, Jüni P, Trelle S. Effectiveness of non-steroidal anti-inflammatory drugs for the treatment of pain in knee and hip osteoarthritis: a network meta-analysis. Lancet (London, England). 2017 Jul 8:390(10090):e21-e33. doi: 10.1016/S0140-6736(17)31744-0. Epub [PubMed PMID: 28699595]
Level 1 (high-level) evidenceMcCabe PS, Maricar N, Parkes MJ, Felson DT, O'Neill TW. The efficacy of intra-articular steroids in hip osteoarthritis: a systematic review. Osteoarthritis and cartilage. 2016 Sep:24(9):1509-17. doi: 10.1016/j.joca.2016.04.018. Epub 2016 Apr 30 [PubMed PMID: 27143362]
Level 1 (high-level) evidenceMurphy NJ, Eyles JP, Hunter DJ. Hip Osteoarthritis: Etiopathogenesis and Implications for Management. Advances in therapy. 2016 Nov:33(11):1921-1946 [PubMed PMID: 27671326]
Level 3 (low-level) evidence